Hospitalised ocular injuries in Osogbo,Nigeria
2015-01-10OlubayoUmarKolawoleMichaelineAsuquoIsawumiOlufunkeAdedolapoOlaopa
Olubayo Umar Kolawole,Michaeline Asuquo Isawumi,Olufunke Adedolapo Olaopa
Department of Ophthalmology,Ladoke Akintola University of Technology University Teaching Hospital,PMB 5000,Osogbo 230221,Nigeria
Hospitalised ocular injuries in Osogbo,Nigeria
Olubayo Umar Kolawole,Michaeline Asuquo Isawumi,Olufunke Adedolapo Olaopa
Department of Ophthalmology,Ladoke Akintola University of Technology University Teaching Hospital,PMB 5000,Osogbo 230221,Nigeria
Received:2015-02-14 Accepted:2015-05-19
·AIM:To describe the epidemiology and outcome ofocular injuries requiring hospital admission in LadokeAkintola University of Technology Teaching Hospital(LTH), Osogbo, Nigeria.
ocular injuries; hospitalisation; visualoutcome; epidemiology; Nigeria
INTRODUCTION
Ocular injuries include all damages caused to the eye and its adnexae,orbital and periorbital tissues by transfer of energy through one of its five forms:chemical,electrical, mechanical,thermal and radiant energy[1].They result from direct contact with stationary or mobile,blunt or sharp objects,hot objects,chemical substances,sources of electrical power and different types of radiation[1].Ocular injuries are recognized causes of permanent anatomical and/or functional complications with their attendant socioeconomic and psychological consequences.The vocational as well as the economic consequences of blindness from ocular injuries areenormous as most of the injuries occur among people in their active years of life.
Available data shows that ocular injuries represented more the cause of a blind eye rather than the cause of a blind person[2].Each year,there are about 55 million eye injuries globally that restrict activities for more than a day. Approximately 19 million persons have at least unilateral permanent reduction in vision and 1.6 million are blinded from ocular injuries[3].Worldwide,about 750 000 cases of ocular injuries are hospitalized every year[3].
Studies from various countries in Africa suggested that ocular injuries occurred frequently in domestic settings,affecting male children and young adults more than any other groups[4,5].Ocular injuries in Nigeria demonstrates geographical variations[6-9],and different internecine, religious and political conflicts in different parts of the country has contributed significantly to causation of ocular injuries in the country[10].
The premorbid status of the eye,the severity of the initial lesion/pathology,the first aid treatment provided,the time elapsed from injury to definitive care and the quality of care are the five major factors associated with final visual outcome of an injured eye[2].
Most of the studies on ocular injuries in South Western Nigeria have either focused on a particular aspect of ocular injuries or a specific age group.Few studies have really documented causes and outcome of moderate to severe ocular injuries that warranted hospitalization.
The aim of this study was to describe epidemiology and outcome of ocular injuries requiring hospitalization in Ladoke Akintola University of Technology Teaching Hospital(LTH), Osogbo,Nigeria over a 12-year period.
SUBJECTS AND METHODS
All patients with ocular injuries who were admitted at LTH, Osogbo between April 2002 and March 2014 comprised the study subjects.They were identified by examining the registers in the Eye Ward and Operation Room.
The charts of all patients who met the inclusion criteria were reviewed and relevant information such as age,sex, occupation,date of presentation,duration of injury before presentation,cause of eye injury,where injury occurred, activity during injury,laterality of the injury,parts of the eye injured,complications of the injury and treatment given were extracted and entered into a form designed for the purpose of this study.Visual acuities during presentation,at discharge and during the last hospital visit were recorded in the Snellen's notation and converted to the decimal notation for ease of analyses.No perception of light(NPL)was assigned the value of zero.In addition,visual acuities at last hospital visit were categorized into good(0.33-1.00),borderline(0.10-0.25)and poor outcomes(<0.10)using the WHO Expert Group's recommendations on Blindness Prevention Outcomes[11].All ocular injuries except those resulting from chemical and thermal burns were classified according to Birmingham Eye Trauma Terminology(BETT)system[12].

Table 1 Socio-demographic characteristics of patients
Data ManagementAll information collected were entered into Statistical Package for Social Sciences(SPSS,Inc., Chicago,IL,USA)version 20 software,cleaned and subsequently analyzed.Frequency and percentages were used to present categorical data while median and range were used to summarize quantitative data.Logistic regression analysis was used to assess effects of different variables on the visual outcome.P<0.05 was taken as statistically significant.
RESULTS
Socio-Demographic Characteristics of the PatientsOne hundred and twenty-seven patients with varying degrees and types of ocular injuries were hospitalized at LTH between April 2002 and March 2014.This represented 12.5%(127/ 1014)of all admissions to the Eye Ward of LTH during that period.These patients comprised 92 males and 35 females (male:female=2.6∶1).The median age at presentation was 22.0y(range:0.5-70.0)while 53(41.7%)patients were children aged less than 16.About one-half of the patients (52.0%)were students.Other socio-demographic characteristics of the patients were as shown in Table 1.
The left eye only was injured among 69(54.3%)patients and the right eye only was injured among 54(42.5%) patients;both eyes were injured in 4(3.1%)patients. Seventy-four(58.3%)patients presented to LTH within 24h of injury and 108(85.0%)were seen by the ophthalmic personnel the same day that they presented at the hospital. For those who had surgery as part of their management,the median interval between presentation and surgery was 3d.The median period of hospitalization was 9.2d while patients were followed up for a median period of 18.9wk after being discharged from the hospital.
Majority of the ocular injuries(35.2%)occurred within the home setting(63.6%of injuries at home involved children), 25.6%at the workplace,19.2%on the road while 16.8% occurred at school.Thirty-two(25.2%)persons injuredtheir eyes while playing and 93.6%of injuries sustained at play involved children.

Table 2 Ocular injuries type by gender
Various objects were responsible for ocular injuries among these patients.Sticks,including canes,broomsticks and plant twigs inflicted injuries on the eyes among 35(27.6%) patients,metals among 20(15.7%)patients;glass and broken bottles were the cause of eye injuries among 13 (10.2%)patients.Different objects comprising fist,goat horn,fire crackers,gun burners,concrete wall,belt and chair inflicted injuries on the eyes among 59(46.5%) patients.It is noteworthy that none of the patients hospitalized for ocular injuries wore any protection during the incident.
The various types of injuries sustained by 127 patients who were hospitalized for ocular trauma at LTH,Osogbo were as presented in Table 2.
Table 3 summarised the visual status of affected eyes at presentation,discharge and last follow up.Among the 116 patients with documented presenting visual acuity,the median visual acuity was 0.00015(3/20000).According to WHO standard,89(76.7%)patients were blind in the affected eyes and only 10(8.6%)had normal vision in the affected eyes at presentation.Median visual acuity in the affected eyes at discharge and at the last follow up visit was 0.005(10/ 2000).Median visual acuity in the fellow eyes of the injured patients was 1.00(20/20).
M anagementVarious treatment modalities were deployed in managing patients in this series as presented in Table 4. Conservative treatment alone was given to 38(21.2%)of the patients.Evisceration was offered to 10(8.5%)patients who had badly traumatized eyes that could not be repaired. Anterior chamber(AC)wash-out was done for 5(4.2%) patients whose hyphaema failed to resorb.Various kinds of repairs with or without lens wash-out,cataract surgery, trabeculectomy and intraocular foreign body(IOFB)removal were carried out among 64(54.2%)patients.
Visual Outcome after ManagementAfter varying interventions,the outcome was good in 21.6%and poor in 67.0%of 97 patients whose records were available as at last follow up visit.Only 6 eyes with good visual outcome suffered open globe injury(OGI)while majority of the eyes with poor visual outcome(49/65)suffered OGI(Table 5).
Factors Associated w ith Poor Visual OutcomePatientswho suffered OGIs were about 9 times more likely to have poor visual outcome compared to those who did not.This association was statistically significant at 5%(Crude OR= 9.16;95%CI:3.43-24.54).Similarly,there was a statistically significant association between blindness at presentation and poor visual outcome(Crude OR=13.24; 95%CI:3.86-45.16).In addition,visual acuity at the last visit correlated with visual acuity at presentation(Kendall's tau-b correlation coefficient=0.609;P<0.05).When the 2 variables were modelled into a logistic regression,there were still significant associations between them and poor visual outcome.The adjusted OR for OGIs and blindness at presentation were 10.84(95%CI:3.43-34.24)and 16.38 (95%CI:4.03-66.46)respectively.

Table 3 Visual status of affected eyes at presentation, discharge and last follow up
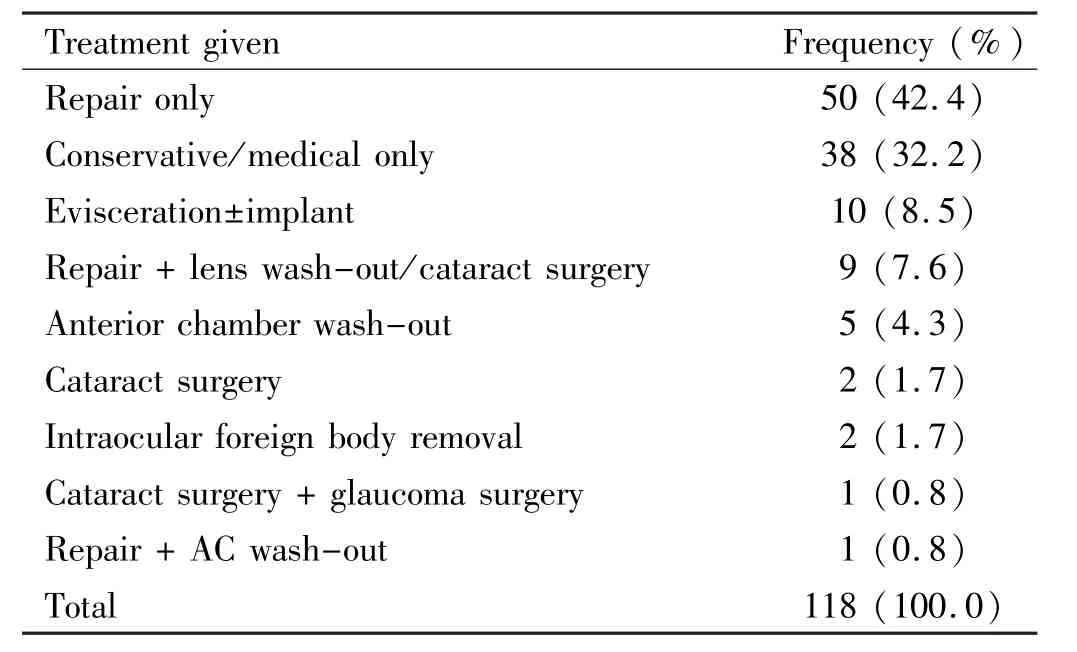
Table 4 Summary of treatment given to the patients
Gender,marital status,injured eye,age at presentation,time interval between injury and presentation or delay in surgical intervention was not significantly associated with poor visual outcome.
As at the last clinic visit,most of the patients with poor visual outcome(59.3%)had corneal scars close to the visual axis, a few(68.7%)had cataracts or lenses that are not visible because of scars.There was no view of the fundus in 81.5%. Some had concomitant vitreous haemorrhage(6.2%),retinal detachment with vitreous haemorrhage(4.6%),retinal detachment only(3.1%)and retinal detachment and choroidal detachment(1.5%)as revealed by ocular ultrasonography.Ten patients(14.3%)had anophthalmic sockets following evisceration.
DISCUSSION
The rate of hospitalization for ocular injuries in this series was about 7.02 patients/100000·y-1based on the population of Osogbo which was 156 694 according to 2006 populationcensus[13].This rate was quite lower than 18.0/100 000·y-1, 53.6/100 000·y-1and 12.6/100 000·y-1that were earlier reported from United States[14],Australia[15]and Singapore[16]respectively.The rate was however much greater than 1.96/ 100 000·y-1,and close to 8.3/100 000·y-1reported from Scotland[17]and Tanzania[18]respectively.LTH has a relatively smaller eye unit than centres where these reported studies were conducted.In addition,many patients with ocular injuries requiring hospitalization might have sought help from traditional healers and other alternatives as is the practice in these parts of the world.

Table 5 Visual outcome of intervention for ocular trauma,LTH,Osogbo
In this series,hospitalised ocular injuries comprised 12.5% of all admissions into the eye wards of LTH.This was far less than the figure reported from a South African hospital,St. John's Eye Hospital,Soweto[19]where 40%of all admission were related to ocular injuries.The hospital was known to be the largest ophthalmic facility in Africa,and this fact might account for the large proportion of hospitalized ocular injuries there.
The median age at presentation in our series was 22.0y,and this was consistent with average age at presentation reported by other workers[7].However,there were variations in the proportion of children admitted for ocular injuries in the different series.In this study,children aged 0-15y constituted 41.7%of patients hospitalized for ocular trauma. There is therefore the need to put up preventive mechanisms and adequate supervision of children during play at home and in school to reduce ocular injuries among them.The adults also need to wear protective devices while working in order to reduce the occurrence of ocular injuries.None of the patients with ocular injuries in our series wore any form of protective device at the time of injury.
Males had higher predilection for severe ocular injuries in our series as evidenced by the male/female ratio of 2.6∶1.This was the findings among other workers,though with variations in male/female ratios reported[5,7,14,16,17].Males are more active,aggressive and have higher tendency to be involved in risky behaviours which make them highly susceptible to injuries and accidents.
In Nigeria,majority of ocular injuries requiring hospitalization occurred within the home-setting usually during accidents and play.This was corroborated by our findings.Some ocular injuries that required hospital admissions in Nigeria occurred during assault/combat with gun pellets on the streets or during communal clashes,during road traffic accidents and while working on the farms[6-10,20].Analyses of USA Eye Injury databases from 2001-2007 showed that 43%of ocular injuries occurred at home and only 20%took place in the workplace[21].A review of penetrating eye injuries managed at Birmingham and Midland Eye Centre in the UK,Bhogal et al[22]reported that majority(41.2%)occurred at home from tools used in Do-It-Yourself exercises and gardening. However,in some developed countries,most serious ocular injuries that required hospitalization are work-related,and such injuries were inflicted by sharp or blunt tools[23].
In most developed countries with better eye care services and referral system than developing countries,almost all patients with ocular injuries present to the hospitals within 24h.In some African countries,there were delays between the occurrence of eye injuries and admission because many patients sought traditional and folk medicines before coming to the hospitals[18].In our series,more than half of the patients (59.2%)presented to the hospital within 24h.In Singapore[16],55.6%of patients presented to eye emergencies within 24h of sustaining injuries.Elsewhere in Africa,the proportion of patients who presented to the hospital within the first 24h of injuries were 7%,12%,and 30% respectively in Tanzania[18],Egypt[5]and Ghana[24].Patients should be educated on the importance of prompt presentation to eye hospitals after sustaining ocular injuries.
It is important to note that two-thirds of patients managed for ocular injuries in our series ended up with poor visual outcome.This compares with reports from other studies in the developing countries where there are limited resources and inadequate capacity to deal with serious ocular injuries that warranted hospitalization.In one of the series in the US[21], 50.8%of patients with severe ocular injuries and initial visual acuity less than 20/200 reduced to only 27.1%after treatment.The authors remarked that introduction of parsplana vitrectomies,intravitreal antibiotics and other new developments made this feat possible.
In this study,OGIs and poor initial visual acuity in the injured eyes were associated with poor visual outcome.Most of the patients with poor visual outcome had concomitant pathologies involving the posterior segments such as vitreous haemorrhage, retina and choroidal detachment.Such pathologies required complex anterior segment surgeries and vitreoretinal procedures such as keratoplasty,keratoprosthesis,vitrectomy and removal of retained intraocular foreign bodies which could have improved the visual outcome.Sadly,requisite equipments and personnels were lacking at LTH when these patients were managed.
This study suffered some limitations.The prominent one was its retrospective nature and its inability to identify risk factors for ocular injuries requiring hospitalization in our environment.The small sample size of patients in this report affected the precision of some of our results.
In conclusion,ocular injuries were significant cause of ocular morbidity and hospitalization in Osun State,Nigeria. Personnel development and capacity building in the provision of complex surgeries will enhance good visual outcome after treatment.There is also an urgent need for health education and preventive strategies for ocular injuries.
REFERENCES
1 Gibson JJ.The contribution of experimental psychology to theformulation of safety:a brief basic research.In:Behavioural approaches to accident research.New York,Association for the Aid of Crippled Children,1961.
2 Negrel AD.Magnitude of eye injuries worldwide.J Comm Eye Health1997;10(24):49-53
3 Negrel AD,Thylefors B.The global impact of eye injuries.Ophthalmic Epidemiol 1998;5(3):143-169
4 Grieshaber MC,Stegmann R.Penetrating eye injuries in South African children:aetiology and visual outcome.Eye(Lond)2006;20(7):789-795
5 Soliman MM,Macky TA.Pattern of ocular trauma in Egypt.Graefes Arch Clin Exp Ophthalmol2008;246(2):205-212
6 Fasina O.Epidemiology of penetrating eye injuries in Ibadan:A 10-year hospital-based review.Middle East Afr J Ophthalmol 2011;18(2): 159-163
7 Okoye OI.Eye injury requiring hospitalization in Enugu,Nigeria:A one-year survey.Niger J Surg Res2006;8(1-2):34-37
8 Ajibode HA,Thanni LO,Onabolu OO,Bodunde OT,Otulana TO. The spectrum of eye injuries in Sagamu,Nigeria.West Afr J Med2013; 32(3):220-223
9 Monsudi KF,Ayanniyi AA,Olatunji OF,AbdulFattah I.Penetrating ocular injuries in a Tertiary Health Facility.Am J Med Sci Med 2013;1 (4):66-68
10 Mpyet CD,Alli SK,Wade PD,Agaba B.Ocular injuries in a civilian conflict in Jos.Nig J Ophthamol2004;12(1):10-13
11 Informal consultation on analysis of blindness prevention outcomes.WHO/PBL/98.68.Geneva:World Health Organisation(WHO), 1998:23
12 Kuhn F,Morris R,Witherspoon CD,Mester V.The Birmingham Eye Trauma Terminology system(BETT).J Fr Ophthalmol2004;27(2):206-210
13“Osogbo”,Official website of the state of Osun.http://osun.gov.ng/about/major-towns/osogbo/;2015.09.18
14 McGwin G Jr,Xie A,Owsley C.Rate of eye injury in the United States.Arch Ophthalmol2005;123(7):970-976
15 Raymond S,Jenkins M,Favilla I,Rajeswaran D.Hospital-admitted eye injury in Victoria,Australia.Clin Experiment Ophthalmol 2010;38 (6):566-571
16 Wong TY,Tielsch JM.A population-based study on the incidence of severe ocular trauma in Singapore.Am J Ophthalmol1999;128 (3):345-351
17 Morris DS,Willis S,Minassian D,Foot B,Desai P,MacEwen CJ. The incidence of serious eye injury in Scotland:a prospective study.Eye (Lond)2014;28(1):34-40
18 Abraham DI,Vitale SI,West SI,Isseme I.Epidemiology of eye injuries in rural Tanzania.Ophthalmic Epidemiol 1999;6(2):85-94
19 Ormerod LD.Causation and management of microbial keratitis in subtropical Africa.Ophthalmology1987;94(12):1662-1668
20 Ojabo CO,Adeniyi OS,Ogli SA.Farm-related ocular trauma in Makurdi,Nigeria.Niger J Med2012;20(1):114-119
21 Kuhn F,Morris R,Witherspoon CD,Mann L.Epidemiology of blinding trauma in the United States Eye Injury Registry.OphthalmicEpidemiol2006;13(3):209-216
22 Bhogal G,Tomlins PJ,Murray PI.Penetrating ocular injuries in the home.J Public Health(Oxf)2006;29(1):72-74
23 Saeed A,Khan I,Dunne O,Stack J,Beatty S.Ocular injury requiring hospitalisation in the South East of Ireland:2001-2007.Injury 2010;41(1):86-91
24 Gyasi M,Amoaku W,Adjuik M.Epidemiology of hospitalized ocular injuries in the upper East Region of Ghana.Ghana Med J2007;41(4): 171-175
尼日利亚奥索波眼外伤患者住院分析
Olubayo Umar Kolawole,Michaeline Asuquo Isawumi, Olufunke Adedolapo Olaopa
(作者单位:尼日利亚,奥索波230221,Ladoke Akintola科技大学附属医院,眼科)
Olubayo Umar Kolawole.bayoteju@gmail.com
目的:分析尼日利亚奥索波Ladoke Akintola科技大学附属医院住院眼外伤患者流行病学及预后。方法:回顾性分析我院2002-04/2014-03所有眼外伤住院患者。患者信息从患者记录中提取并录入预设表格,采用SPSS 20对数据进行统计分析。通过Logistic回归分析评估不同变量对患者眼外伤治疗和视功能预后的影响, P<0.05具有统计学意义。结果:共127例患者纳入本研究。平均年龄22(范围:0.5~70.0)岁,男:女比例为2.6:1。大多数眼外伤,约35.2%发生在家里。127例患者中,开放性眼外伤74例(58.3%),闭合性眼外伤34例(26.8%),眼附属器官损伤7例(5.5%),眼球爆裂伤6例(4.7%),眼化学伤4例(3.1%),眼内异物及眼外伤各1例。本研究中2/3眼外伤患者经治疗,视功能预后仍不佳。初诊视力低下(OR= 13.24)和开放性眼外伤(OR=9.16)与视功能预后不佳具有显著相关性。结论:发展中国家急需健康教育及眼外伤预防措施。同时,需增强行复杂性眼外伤前后段手术的能力,以改善严重眼外伤患者的视功能预后。
眼外伤;住院治疗;视功能预后;流行病学;尼日利亚
Olubayo Umar Kolawole.Department of Ophthalmology,College of Health Sciences,Ladoke Akintola University of Technology,P.O.Box 2570,Osogbo 230221, Nigeria.bayoteju@gmail.com
10.3980/j.issn.1672-5123.2015.11.02
:Kolawole OU, Isawumi MA, Olaopa OA. Hospitalisedocular injuries in Osogbo, Nigeria. Guoji Yanke Zazhi(Int Eye Sci)2015;15(11):1842-1846
引用:Kolawole OU,Isawumi MA,Olaopa OA.尼日利亚奥索波眼外伤患者住院分析.国际眼科杂志2015;15(11):1842-1846
·METHODS:Retrospective chart review of all patientshospitalized for ocular injuries at LTH, Osogbo betweenApril 2002 and March 2014 was undertaken. Informationextracted from patients records were entered into a predesignedform. Data were analyzed with StatisticalPackage for Social Sciences (SPSS) version 20. Logisticregression analysis was used to assess effects of differentvariables on the visual outcome of ocular injuries aftertreatment among the subjects. P<0. 05 was used as test ofstatistical significance.
·RESULTS:One hundred and twenty - seven patientswere hospitalized at LTH within the study period. Themedian age was 22. 0y ( range: 0. 5 - 70. 0 ) and male: female ratio 2. 6 ∶ 1. Majority of the injuries (35. 2% ) occurred within the home setting. Of the 127 patients, 74(58. 3% ) had open globe Injuries (OGI), 34 (26. 8% ) hadclosed globe injuries ( CGI ), 7 ( 5. 5% ) had adnexalinjuries, 6 (4. 7% ) had ruptured globes, 4 (3. 1% ) hadchemical injuries, 1 (0. 8% ) patient each had retainedintraocular foreign body and thermal eye injury. Two -thirds of patients managed for ocular injuries in this serieshad poor visual outcome. There were statisticallysignificant associations between poor initial visual acuity(OR = 13. 24) and OGI with poor visual outcome (OR =9. 16).
·CONCLUSION: There is an urgent need for healtheducation and, to put in place preventive strategies forocular injuries. Developing countries need to build upcapacity to offer complex anterior and posterior segmentsurgeries for those with severely injured eyes so as toimprove the visual outcomes.
