放射状冲击波疗法在电脑所致重复性使力损伤中的治疗作用:前瞻性单盲随机对照研究
2015-01-05王旭明邢更彦李志国云南省蒙自市武警8750部队医院骨外科蒙自6699北京武警总医院骨科中心北京00039
王旭明,邢更彦,李志国.云南省蒙自市武警8750部队医院骨外科,蒙自 6699;.北京武警总医院骨科中心,北京 00039
放射状冲击波疗法在电脑所致重复性使力损伤中的治疗作用:前瞻性单盲随机对照研究
王旭明1,邢更彦2,李志国2
1.云南省蒙自市武警8750部队医院骨外科,蒙自 661199;2.北京武警总医院骨科中心,北京 100039
目的评价低能量放射状体外冲击波疗法在电脑所致重复性使力损伤中的疗效。方法采用前瞻性单盲随机对照研究的方法,应用瑞士EMS Dolorclast放射状冲击波治疗机电脑所致重复性使力损伤82例,随机分为研究组和对照组,每组病例41例。研究组以痛点为中心,行体外冲击波治疗,治疗处方为:压力2.0 bar,能量0.08 mJ/mm2,频率2 000次,治疗时间3至5周;对照组治疗处方为压力2.0 bar,能量0.08 mJ/mm2,频率20次,
电脑所致重复性使力损伤;冲击波;治疗
1 Introduction
Computers are now important to human teaching and research,with many professions using them on a daily basis for long sessions of word processing,email,Web browsing,and more.RSI(also known as repetitive stress injury,cumulative trauma disorder (CTD),upperextremity musculoskeletaldisorder (UEMSD),occupational overwork syndrome.etc)[1]remains a controversial topic,is an injury of the musculoskeletal and nervous systems that may be caused by repetitive tasks,forceful exertions,vibrations,or sustained or awkward positions[2].RSI was first diagnosed in Australia in the 1980’s.The number of RSI cases are increasing,because more people are specializing in jobs that require them to repeat the same movements hour after hour.While keyboard and mouse users are especially at risk. Although numerous therapies are advocated in the management of computer-related RSI,these can be ineffective,temporary and not be able to cure entirely. As a result,new treatment options are being sought. Theapplication ofrESWT in thetreatmentof computer-related RSI is not covered yet[1-4].
Extracorporeal shock wave therapy is an increasingly populartherapeuticapproach to the treatment of pseudoarthrosis and delayed or non union of fracture,as well as in the treatment of a number of soft tissue complaints[5].Extracorporeal shock waves are single pressure pulses of microsecond duration that can be focused upon a site using ultrasound guidance. In the radial extracorporeal shock wave therapy,the shock wave is produced pneumatically through the acceleration of a projectile inside the handpiece,unlike the ESWT where the shock wave is produced by electrohydraulic,piezoelectric and electromagnetic systems. Pressure waves generated by pneumatic mechanism are transmitted radially from the tip of applicator to the target zone,decreasing in energy proportional to the third power of the penetration depth in the tissue[6]. Radial ESWT has been introduced into medicine as an effective and easy method to apply shock wave technology[7].In this study,it's reported the application of rESWT in computer-related RSIs,using a prospective randomized controlled single-blind study.
2 Methods
From October 2010 to May 2015,82 adult subjects with a clinical diagnosis of computer-related RSI were recruited in the out-patient clinic after assessment by a qualified orthopedist and physiatrist. Informed consent was obtained by all subjects prior to participation.
There were 58 men and 24 women with a mean age of 34 years(range 18-53).All forms of RSI are present as a result of frequent use of computer keyboards and mice.
The inclusion criteria were:the presence of persistent back pain,neck pain,shoulder pain,hand/ wrist pain,arm pain,and finger pain etc,refractory to conservative treatment,provided for at least one month,including NSAIDs,physicaltherapy and immobilisation of afflicted part during the acute phase of pathology.At least 2 weeks before RSWT wasdone,the abovementioned therapieswere discontinued.All subjects had normal X-rays/bloods and MRIs,but had abnormal nerve conduction.
Exclusion criteria were:some general contraindications for shock wave treatment,such as recent trauma and localinfection,cardiac arhythmia,pacemaker implant,lung tissue in direction of sound,coagulopathy, pregnancy, arthritis, neurological abnormalities,diabetes,vasculitis and malignancy;several confirmed cervical spondylosis,cervical disc herniation,scalenus syndrome,neurofibroma-tosis,and syringomyelia.
The radiallow-energy shock wave therapy (Swiss DolorClast®,EMS Medical GmbH;EFD= 0.08 mJ/mm2)was administered to the patient's trigger points without local anaesthesia.The shock wave applicator was positioned over the area of maximum tenderness as reported by the patient or biofeedback. There is no consensus on appropriate dose of shock wave and treatment parameters remain empirical. However,1 000 to 2 000 impulses of an EFD from 0.01 up to 0.28 mJ/mm2are usually recommended and applied 3 times at weekly intervals in musculoskeletal disorders.The treatment with lowenergy shock wave is recommended for patients with tendinopathies[8].All patients in the study group had 3 sessions,2000 impulses for each session of RSWT that were applied using a 15 mm applicator,a pressure and a frequency was 2.5 bar and 8 Hz.All patients in the control group had 3 sessions,20 impulses for each session of RSWT that were applied using a 15 mm applicator,a pressure and a frequency was 2.5 bar and 8 Hz.The machine makes a noise with every shock wave delivered.The treatment area was prepared with coupling gel to minimize the loss of shock wave energy at the interface between applicator tip and skin.Side effects such as skin irritation,petechiae,haematomas or swelling were observed in only 10 patients.During the treatment,no other treatments were carried out and the patients were instructed to work as usual after each shock wave treatment.
All patients were evaluated 3 times:before therapy(pre-treatment),at the end of therapy(posttreatment) and to 3 months (follow-up).The examination consisted of assessment of pain and functional impairment level.All subjects’symptoms were specified with a VAS ranging from 0,no pain to 100,maximal pain during the day and at night. Functional impairment level was assessed with the disabilities of the arm,shoulder,and hand(DASH) questionnaire developed by the Upper Extremity Collaborative Group(UECG)[9].The outcome was considered to be excellent if there was a reduction of pain by VAS between the80.0 and 100.0,a resumption of working activity without limitations. The outcome was considered as good,if the reduction of pain was between 60.0 and 79.9,working activity was resumed with mild limitation.The outcome was considered fair if there was a reduction of pain by VAS between 30.0 and 59.9,a resumption of working activity with moderate limitations.The cases were considered poor when a reduction of pain was not referred,resumption of working activity with severe limitation.A 2-sample t test was applied to compare the differences of the baseline data and the subsequent data at the same time point between two groups.A 2-way analysis of variance(ANOVA)was used within each group before and after treatment and 3 months follow-up.All data was analyzed by SPSS 18.0.Statistical significance was set at a P value of<0.05.
3 Results
Eight-two subjects were recruited to the clinical study and their characteristics are detailed in table 1. The baseline characteristics were similar and without statistic significance in both groups.There have been no withdrawal,82 patients had completed the study. No other adverse effects were reported.
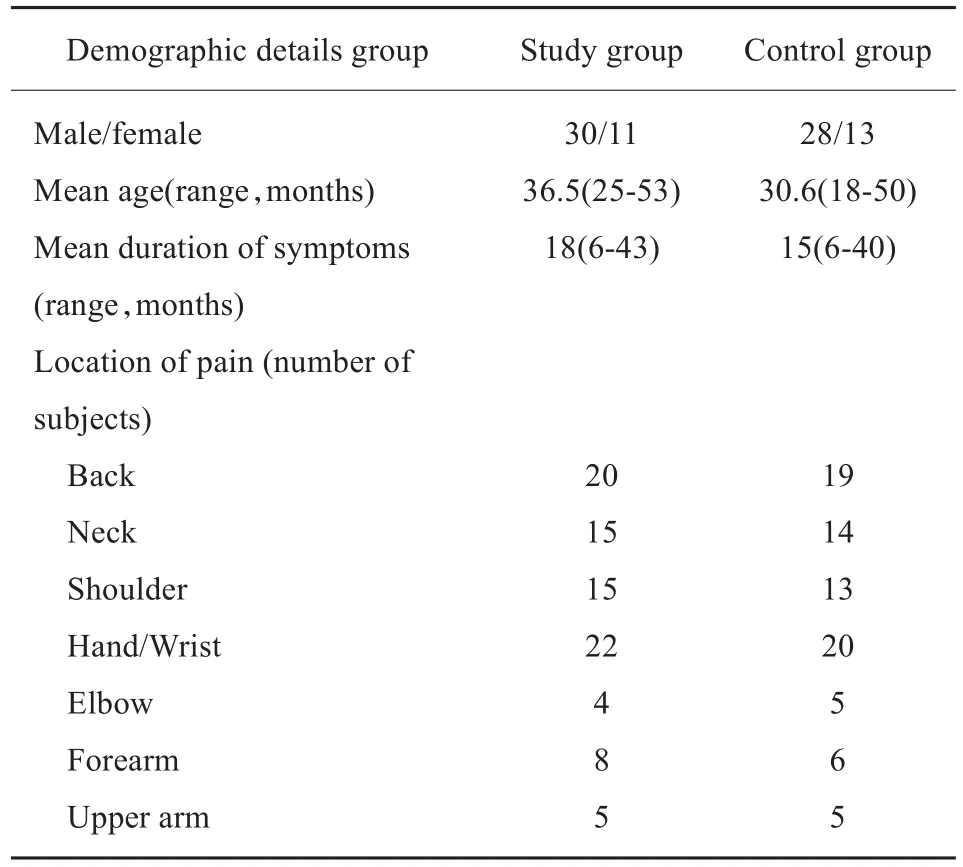
Tab.1 Baseline characteristics of all subjects表1 电脑所致重复性使力损伤患者基本信息
The mean pain-score was shown in table 2.There was no statistic significance in both groups before treatment(P=0.514).Post-hoc comparison demonstrated a significant differences between study and control groups after treatment(P=0.017)and at 3 months follow-up(P<0.001).In the same group,before and after treatment,a statistically significant reduction was shown in the study group(P<0.001) and no significant difference found in the control group.

Tab.2 Visual analogue scale for pain in both groups during the study(mean(SD,range))表2 研究期间两组患者VAS评分情况(平均值(标准差,范围))
The mean value of DASH functional impairment in both groups before treatment was shown in table 3. There was no statistic significance at baseline(P= 0.742). Post-hoc comparison demonstrated a significant differences between study and control groups(P<0.001)after treatment and at the 3 months follow-up.In the same group,before and after treatment,a statistically significant reduction was shown in the study group (P<0.001)and no significant difference found in the control group.

Tab.3 The mean values of DASH functional impairment scale in the Study and Control Groups(mean(SD,range)表3 治疗前后上肢功能评分情况(平均值(标准差,范围)
There were 24,31 good or excellent results in the study group compared with only 8,10 in the control group after treatment and 3 months follow-up. The rate of good and excellent outcomes according to the relief of pain and improvement of function was significantly(56%,76%)better in the study group than in the control group after treatment and 3 months follow-up respectively.

Tab.4 Overall outcome in both groups after treatment and 3 months follow-up表4 体外冲击波干预后总体效果评判
4 Discussion
RSI now makes up more than 60 percent of work-related illnesses[1].As more and more work,vocation and recreation involves computers,everyone needs to be aware of the hazard of RSI to the hands,shoulders,backs,and arms resulting from the use of computer keyboards and mice.Actually,RSI is not like a diagnosis,but a term used to describe a very complicated,many-faceted soft tissue problem[1].Thiscan be a serious and very painful condition that is far easier to prevent than to cure once contracted. Although many treatments of RSI are recommended,shock wave therapy in RSI is not reported.
Generally speaking,no organic disorders happen to anyone who has RSIs.Goals of treatment are pain relief and restoration of function.Immediate pain reduction led to early return to better normal work. Based on the scores of the DASH modules including symptoms,function and sport,this follow-up study of 82 RSI subjects evaluated impairments and disabilities perceived 3 times during the study.The Disability of Arm,Shoulder and Hand questionnaire is a standardized measure which captures the patients’own perspective of their upper body health status.Jester,et al[10].also confirmed that the DASH was a useful instrument for outcome evaluation and DASH had potential in the development of patient-centred treatmentprogrammes which are tailored to the individual patients’requirements and have relevance to their daily activities.
ESWT is becoming increasingly popular as a therapeutic option in the treatment of a variety of musculoskeletal complaints, including lateral epicondylitis[11-12],chronic proximal plantar fasciitis[13],calcific tendonitis of the shoulder[14],and has a positive effect.The Radial Extracorporeal Shock Wave Therapy for the treatment of computer-related RSI in medicine is a new,promising method.As ESWT is a non-invasive method with no serious side effects,it is also an excellent alternative method. Additionally,the results show that radial shock waves are able to induce analgesia in the treated area and improve upper limbs’function.
Compared with focused shock wave applicators,rESWT devices address larger treatment areas,thus providing potential advantages in superficial applications like tendinopathies and skin conditions. For deep soft tissue treatments or bone injuries,the radialtechnique has some limitations regarding penetration depth and higher energy levels[15-16].In contrast to so-called focused shock wave therapies,the radial technique is used to treat the superficial painful region rather than a deep painful area.It is well known that RSI originates from a painful area rather than a deep certain locally limited spot.
In our study,radial shock waves were oriented without anesthesia by patient-guided feedback to the point of maximum tenderness.Rompe et al had demonstrated that local anesthesia may inhibit direct analgesic effects like the modification of the release of pain mediators,hyper-stimulation,and the gatecontrol mechanism.ESWT applied without local anesthesia wassignificantly more effective than ESWT used with local anesthesia[17].Treatment was applied without anesthesia, and our results demonstrated rESWT to besafewith excellent tolerability.So far,to our knowledge,this protocol of treatment has not been analysed previously in a clinical setting.The authors think that the low-energy rESWT is effective for patients suffering from RSI and overall pain modulation,thus allowing daily activity and having a positive improvement in upper body by the values of DASH functional impairment scale.
The shock waves are used to provoke painful levels of stimulation to relieve pain,by so-called hyper-stimulation analgesia[18].The exact mechanism of reducing pain by shock wave therapy is still on study.The intensity of pain was always lower in the following sessions.This effect seems to be related to inhibition of pain receptors or denervation[19].Some studies have found that shock wave seems to distort axonal contents,increasing the permeability and leading to depolarization.So the nociceptors loose their ability for generation of potentials necessary to elicit the pain signal response[11].Our success with this new method of treatment warrants further study of the most efficient method of its use and the mechanism of its influence on pain.
OurresultssuggestthatRSWT effectively reduces pain (improvement of VAS scores)and increases upper extremity function(improvement of DASH functional measurements,as well as quality of life) without device-related adverse effects. Moreover,the results seen after the treatment were maintained over the following 3 months.
Even with the limitation of a short follow-up and a small scale of computer-related RSIs,the results of study show the effectiveness and safety of shock waves in the treatment of patients suffering RSIs.In fact,computer-related RSIs yet include eye strain,anterior knee pain and Pilot seat syndrome,and so on. Such RSIs need to be addressed in further studies in the future.The success of this treatment however,warrants further well designed prospective control studies,with a long term follow-up in order to define the optimal number of shock waves applications and the most adequate energy density levels and impulse rate,and to understand better the mechanism of influencing pain symptoms.
[1] Pascarelli E.Pascarelli's complete guide to repetitive strain injury:what you need to know about rsi and carpal tunnel syndrome[M].New Jersey:John Wiley&Sons Inc,2004.
[2] Damany S,Bellis J.It's not carpal tunnel syndrome!rsi theory and therapy forcomputerprofessionals[M].Philadelphia:Simax,2001.
[3] Abelson B,Abelson K.Release your pain:resolving repetitive strain injuries with active release techniques[M].2ndEdition. Canada:North Atlantic Books,2005.
[4] Quilter D.The repetitive strain injury recovery book[M]. Indiana:iUniverse,2008.
[5] Siebert W,Buch M.Extracorporeal shock waves in orthopaedics [M].Berlin:Springer-Verlag Berlin Heidelberg,1997.
[6] Magosch P,Lichtenberg S,Habermeyer P.Radial shock wave therapy in calcifying tendonitis of the rotator ruff-A prospective study[J].Orthop Ihre Grenzgeb,2003,141(6):629-636.
[7] Gerdesmeyer L,Maier M,Haake M,Schmitz C.Physicaltechnical principles of extracorporeal shock wave therapy (ESWT)[J].Orthopade,2002,31(7):610-617.
[8] Rompe JD,Kirkpatric CJ,Kűllmer K,et al.Dose-related effects of shock waves on rabbit tendo Achillis:A sonographic and histological study[J].J Bone J Surg[Br],1998,80(3):546-552.
[9] Hudak PL.Development of an upper extremity outcome measure:the DASH(Disability of the Arm,Shoulder,and Hand)[J].Am J Ind Med,1996,29(6):602-608.
[10] Jester A,Harth A,Wind G,et al.Disabilities of the Arm,Shoulder and Hand (Dash) Questionnaire: Determining functional activity profiles in patients with upper extremity disorders[J].J Hand Surg Eur,2005,30(1):23-28.
[11] Ogden JA,Alvarez R,Levitt R,et al.Shock wave therapy (Orthotripsy)in musculoskeletal disorders[J].Clin Orthop Rel Res,2001,6(387):22-40.
[12] Thiel M.Application of shock waves in medicine[J].Clin Orthop Rel Res,2001,6(387):18-21.
[13] Ogden JA,Alvarez R,Levitt R,et al.Shock wave therapy for chronic proximal plantar fasciitis[J].Clin Orthop Rel Res,2001,6(387):47-59.
[14] Haake M,Deike B,Thon A,et al.Exact focusing of the extracorporeal shock wave therapy for calcifying tendinopathy [J].Clin Orthop Relat Res,2002,4(397):323-331.
[15] Gerdesmeyer L,Maier M,Haake M,et al.Physical-technical principles of extracorporeal shock wave therapy(ESWT)[J]. Orthopade,2002,31(7):610-617.
[16] Gerdesmeyer L,Schrabler S,Mittelmeier W,et al.Tissueinduced changes of the extracorporeal shock wave[J]. Orthopade,2002,31(7):618-622.
[17] Rompe JD,Meurer A,Nafe B,Hofmann A,et al.Repetitive low-energy shock wave application without local anesthesia is more efficient than repetitive low-energy shock wave application with local anesthesia in the treatment of chronic plantar fasciitis[J].J Orthop Res,2005,23(4):931-941.
[18] Melzack R.Prolonged reliefofpain by brief,intense transcutaneous somatic stimulation[J].Pain 1975,1(4):357-373. [19] Haupt G.Use of extracorporeal waves in the treatment of pseudoarthrosis,tendinopathy and other orthopedic diseases[J]. J Urol,1997,158(1):4-11.
The application of radial shock wave therapy in the treatment of computer-related repetitive strain injuries:a prospective randomized controlled single-blind study
WANG Xuming1,XING Gengyan2,LI Zhiguo2
1.Department of Orthopedics,8750 Hospital of the Chinese People's Armed Police Forces,Mengzi 661199,China;2.Orthopedic and Traumatology Unit,General Hospital of the Chinese People’s Armed Police Forces,Beijing 100039,China
ObjectiveTo evaluate the efficacy of the treatment with low-energy radial extracorporeal shock wave therapy(rESWT or RSWT)in computer-related repetitive strain injuries(RSIs).MethodsIn a prospective randomized controlled single-blind study,82 adults with computer-related RSIs diagnosed by a qualified orthopedist and physiatrist were randomly assigned to study group and control group.There were 41 patients in the study group and 41 patients in the control group.Both groups had received a treatment per week for 3-5 weeks;The study group had received on average 2000 pulses of RSWT at pressure of 2.0 bar(8 Hz,0.08 mJ/mm2)according to Swiss EMS DolorClast equipment and the control group 20 pulses of RSWT.All subjects were assessed 3 times:before treatment,at the end of treatment and to 3 months follow-up.Outcome measures consisted of visual analogue scores(VAS)for pain in the day and at night and functional impairment level.The outcome was considered to be excellent if there was a reduction of pain by VAS between the 80.0 and 100.0,and a resumption of working activity without limitations.The outcome was considered as good if the reduction of pain was between 60.0 and 79.9,working activity was resumed with mild limitation.The outcome was considered fair if there was a reduction of pain by VAS between 30.0 and 59.9,a resumption of working activity with moderate limitations.The cases were considered poor when a reduction of pain was not referred,resumption of working activity with severe limitation.ResultsStatistical analysis of VAS,disabilities of the arm,shoulder,and hand(DASH)measures had shown,both after treatment and to the follow-up of 3 months,significant difference comparing study group versus control group(P≤0.017).Eighty-two subjects participated and there were no significant differences between the two groups at baseline.A significant improvement in pain and functions was noted only in the study group after treatment and at 3 months follow-up.The rate of good and excellent outcomes according to the improvement in pain and function was significantly(56%,76%)better in the study group than in the control group after treatment and at 3 months follow up respectively.ConclusionRSWT significantly both relieves pain and improves function and quality of life compared with sham therapy in patients with computer-related repetitive strain injuries.
Computer-related strain injuries;Shock wave;Treatment治疗时间3至5周。对治疗前,治疗后和治疗后3个月的随访。观察指标包括视觉模拟评分(VAS)和功能障碍的水平。结果电脑所致重复性使力损伤经冲击波治疗后的优良率为56%,3个月后随访优良率为76%。结论放射状冲击波治疗电脑所致重复性使力损伤安全、有效。
R873.5
A
2095-378X(2015)02-0089-06
10.3969/j.issn.2095-378X.2015.02.006
王旭明(1979—),男,山东栖霞人,硕士研究生,研究体外冲击波疗法在骨科领域的应用;电子信箱:wxm_ 0606@163.com
