超声评分系统结合血清附睾分泌蛋白4、CA125对卵巢肿瘤的诊断意义
2014-07-19柳英兰刘学宁
张 丹,柳英兰,刘学宁
超声评分系统结合血清附睾分泌蛋白4、CA125对卵巢肿瘤的诊断意义
张 丹1,柳英兰2,刘学宁1
目的 探讨超声评分系统结合血清附睾分泌蛋白4 (human epididymal secretory protein 4,HE4)、CA125检测结果,对卵巢肿瘤的诊断意义。方法 选取卵巢癌78例(卵巢癌组),卵巢良性肿瘤102例(卵巢良性肿瘤组),检测两组血清HE4及CA125水平,以80例健康人为对照组,制作受试者工作特征(ROC)曲线,以曲线下面积(AUC)反映诊断的准确性。对两组患者进行超声评分,分别计算超声评分系统与肿瘤标志物联合对卵巢癌诊断的敏感性、特异性。结果 卵巢癌组血清HE4及CA125水平明显高于卵巢良性肿瘤组和对照组,差异均有统计学意义(P<0.05);卵巢良性肿瘤组与对照组间比较,HE4差异无统计学意义(P>0.05),CA125差异有统计学意义(P<0.05)。HE4诊断卵巢癌的敏感性、特异性分别为94.3%,96.1 %;CA125诊断卵巢癌的敏感性、特异性分别为87.4%,94.2%。HE4联合超声评分系统敏感度为为91.4%;CA125联合超声评分系统为85.7%;HE4、CA125、超声评分系统三项联合检测为96.1%。结论 血清HE4、CA125联合超声评分系统诊断卵巢肿瘤的敏感性最高。
人附睾分泌蛋白;CA125;卵巢恶性肿瘤;超声评分系统
卵巢癌5 年生存率仅为20%左右[1],早期诊断、早期治疗是改善其预后的重要手段。人附睾分泌蛋白4 (human epididymal secretory protein 4,HE4)是新近提出的肿瘤标志物,可用来筛查卵巢癌。CA125是检测卵巢癌的常用标志物,但假阳性率高,Ⅰ期卵巢癌仅有50%~60%的患者CA125值升高,单用CA125阳性诊断率<10%,结合超声检查也只能将阳性诊断率提高到20%[2]。为此,我们将超声评分系统与血清HE4、CA125检测结合,旨在探讨它们对卵巢肿瘤的诊断意义,并期待提高卵巢肿瘤的诊断率。
1 对象与方法
1.1 对象 收集2010-01至2011-12哈尔滨医科大学附属第一医院及武警黑龙江总队医院住院盆腔肿块180例(年龄25~73岁,平均45.3岁)的病历资料。术前均测定血清HE4值及CA125值,应用彩色阴道超声(有5例未婚患者改用腹部彩色超声)对肿块进行评分。术后病理确诊卵巢恶性肿瘤78例(卵巢癌组),良性肿瘤102例(卵巢良性肿瘤组)。随机选取同期健康体检者80例作为对照组,平均(39.7±7.6)岁,均除外肿瘤病史。
1.2 试剂和仪器 RocheE170全自动免疫分析仪为瑞士Roche公司产品,HMGA1试剂盒及质控品,HE4试剂盒及质控品由ADL公司提供,CA125试剂盒及质控品由瑞士Roche公司提供。使用Acuson Sequoia 512,ALOKA- a5彩色多普勒超声诊断仪,阴道探头频率6~7.5 MHz,腹部探头频率2~5 MHz。
1.3 方法
1.3.1 血清HE4及CA125检测 三组均采取空腹静脉血5 ml(取标本前均未经放疗、化疗或其他治疗),收集于试管中,室温下静置30 min,2000 r/min离心15 min后取上清,-80 ℃保存,并避免反复冻融。标本采集前,所有研究对象均填写知情同意书,符合医学伦理学要求。HE4水平的测定采用ELISA方法,采用两项式拟合曲线法绘制标准曲线,如果质控品检测结果在试剂标示值范围内,则认为血清检测结果有效;CA125水平的测定采用电化学发光免疫分析法,标志物水平高于临界值(cut-off值)即判定为阳性。联合检测时任意标志物高于临界值即判定为阳性。
1.3.2 超声检测方法及标准 对已婚妇女术前经阴道彩色多谱勒超声检查,计算血流阻力指数(RI)、搏动指数(PI)值,根据二维超声的声像图特点及彩色多普勒血流特点、参数,参照Valentin 、Sasson 、Finkler 、Lerner 、Weber Juan[3-8]的评分系统,总结出超声评分系统,评分内容为:形态规则(0分),不规则(1分);包膜完整(0分),不完整(1分);隔厚<3 mm(0分),≥3 mm(1分);周边血流情况Ⅰ型(0分),Ⅱ型(1分),Ⅲ型(3分);RI>0.43(1分),RI ≤0.43 (2分);PI>1.0 (1分),PI≤1.0 (2分); 腹水有(0分), 无(2分)。每项指标得分相加得出每个肿瘤的最后超声积分.积分<4 分诊断良性肿瘤,积分≥4 分诊断为恶性肿瘤。

2 结 果
2.1 各组HE4、CA125检测水平 卵巢癌组血清HE4及CA125水平明显高于卵巢良性肿瘤组和对照组,差异均有统计学意义(P<0.05);卵巢良性肿瘤组与对照组间比较,HE4差异无统计学意义(P>0.05),CA125差异有统计学意义(P<0.05)。见表1。HE4诊断卵巢癌的敏感性、特异性分别为94.3%,96.1 %;CA125诊断卵巢癌的敏感性、特异性分别为87.4%,94.2%。
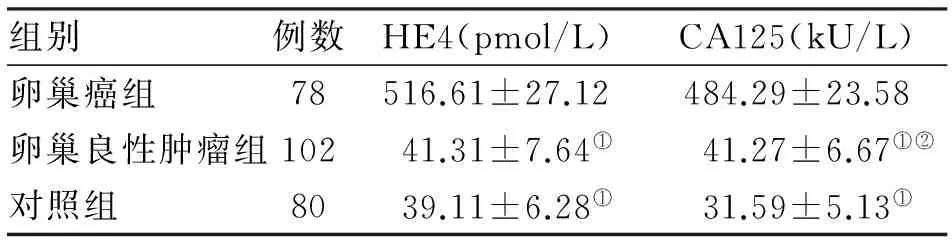
组别例数HE4(pmol/L)CA125(kU/L)卵巢癌组78516.61±27.12484.29±23.58卵巢良性肿瘤组10241.31±7.64①41.27±6.67①②对照组8039.11±6.28①31.59±5.13①
注:与卵巢癌组比较,①P<0.05;与对照组比较,②P<0.05
2.2 卵巢良、恶性肿瘤的超声二维特征及彩色血流信号分布特点 卵巢良性肿瘤的超声特征:囊性多见,边界清,包膜完整,囊性部分有细分隔,少部分有乳头,囊液透声好多见,周边隔上及实性部分多无血流显示(图1A)。卵巢癌超声特征:囊实性多见,包块边界多不清,包膜不完整,瘤内有粗细不均的多个分隔,分隔上有乳头,实质内及包膜上多见血流信号(图1B)。
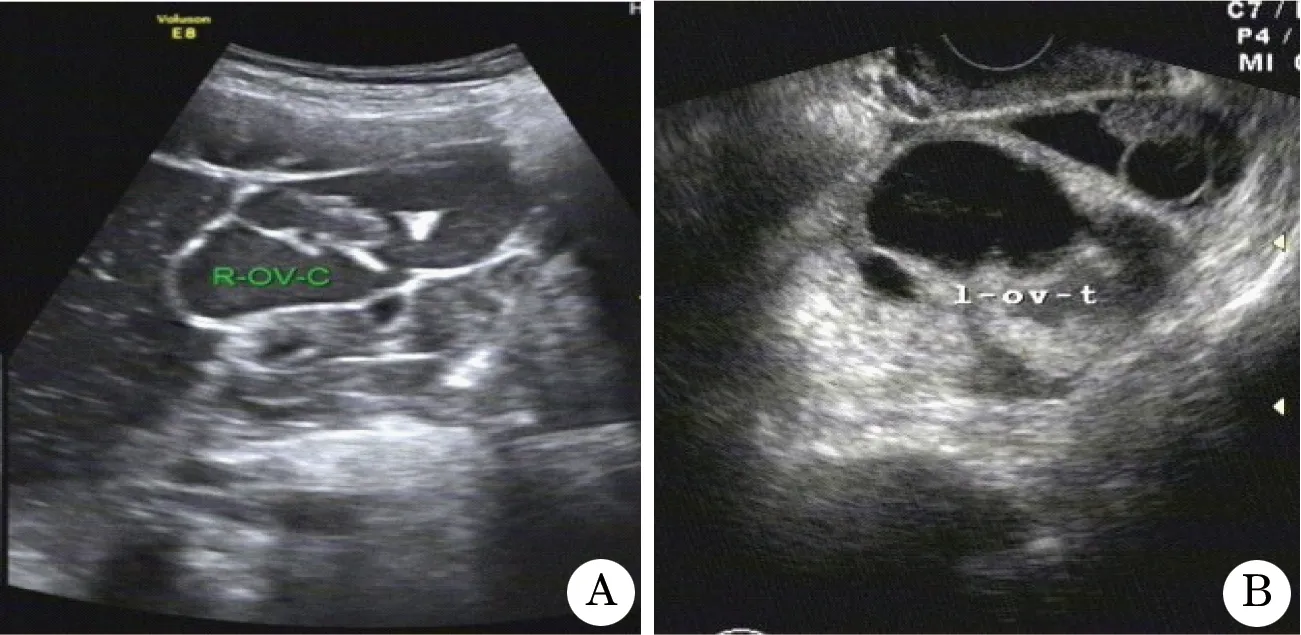
图1 卵巢肿瘤超声检查
良性肿瘤组中,Ⅰ型血流97例,Ⅱ型5例,Ⅲ型0例;卵巢癌组中,Ⅰ型血流2例,Ⅱ型21例,Ⅲ型55例。卵巢癌组RI为0.387±0.103,PI为0.624±0.212;卵巢良性肿瘤组RI为0.652±0.186,PI为0.845±0.154,两组各指标比较差异均有统计学意义(P<0.05)。超声评分系统对卵巢癌诊断的敏感性为91.2%,特异性为75.1%;对卵巢良性肿瘤诊断的敏感性为86.7 %,特异性为83.5 %。
2.3 血清HE4、CA125水平及超声评分系统的相关性分析 卵巢良性肿瘤组、对照组血清HE4和CA125水平无相关性(P>0.05),卵巢癌组血清HE4和CA125水平呈正相关(r=0.43,P<0.05)。以卵巢良性肿瘤组为参照,卵巢癌组血清HE4、CA125、超声评分系统检测的AUC分别为0.925、0.784、0.675,生物敏感度分别为91.6%、85.7%、73.6%。HE4联合超声评分系统敏感度为91.4%;CA125联合超声评分系统为85.7%;HE4、CA125、超声评分系统三项联合检测为96.1%。
3 讨 论
本研究表明,超声评分系统对卵巢良恶性肿瘤诊断有一定的敏感性和特异性,与陈光等[10]报道结果一致。建议在使用超声评分系统的同时联合使用血清肿瘤标志物,以增加对卵巢癌诊断的特异性。另外,RI诊断卵巢癌的敏感性、特异性均高于PI,但在一部分卵巢恶性肿瘤中RI值无明显减低,其敏感性不如血清HE4和CA125。
HE4最早于1991年被Kirchhoff等[9]发现存在于附睾上皮组织, 为小分子分泌型糖蛋白, 在卵巢癌患者血清、组织和卵巢癌细胞株上清中均可检测到。HE4在正常卵巢组织不表达,却在卵巢癌组织中大量表达。本研究显示,在95.0%的特异度下,HE4诊断卵巢癌的敏感度较高(86.7%),与Shah等[11]报道基本一致。提示HE4作为卵巢癌诊断的标志物敏感度高于CA125(73.6%),因而HE4在预测卵巢癌准确性上优于并独立于CA125和超声评分系统,可作为卵巢癌诊断更为敏感的肿瘤标志物,并可替代CA125对卵巢癌进行早期诊断及术后随访和复发监测。
本研究表明,HE4、CA125与超声评分系统结合可增加对卵巢癌诊断的敏感性,最高达96.1%,从而大大提高对卵巢癌诊断的准确性,降低漏诊率。
[1] Whitehouse C, Solomon E. Current status of the molecular characterization of the ovarian cancer antigen CA125 and implications for its use in clinical screening [J]. Gynecol Onco, 2003, 88: 152-157.
[2] Cohen L S, Escobar P F, Scharm C,etal. Three dimension al power doppler ultrasound improves the diagnostic accuracy for ovarian cancer prediction [J] . Gynecol Onco, 2001, 84(2) : 352-353.
[3] Valentin L.Limited contribution of Doppler velocimetry to the differential diagnosis of extrauterine pelvic tumors[J].Obstet Gynecol,1994,83:425-433.
[4] Sasson A M,Timor I E,Antner A,etal.Transvaginal sonographic characterization of ovarian diseases: Evaluation of a new scoring system to predict malignancy[J].Obsetet Gynecol,1991,78:70-76.
[5] Finkler N I,Benacerraf B I,Lavin P,etal.Comparison of serum CA125, clinical impression and ultrasound in the preoperative evaluation of ovarian masses[J].Obstet Gynecol,1988,72:659-663.
[6] Lerner J R,Timor I E,Fedeman A,etal.Transv -aginal ultrasonographic characterization of ovarian masseswith an inproved,werghted scoring system [J].Am J Obstet Gynecol,1994,170:81-87.
[7] Weber G,Merz E,Bahlmann F,etal.A new so Nnomorphologic scoring- system (Mainz score)for the assessment of ovarian tumors using transvaginal ultrasonography[J].Ultraschall Med,1999,20(1):2-8.
[8] Juan L.A newscoring systemto differentiate benign from nalignant adnexal masses[J].Am J Obstet Gynecol,2003,34(4):685-697.
[9] Karlsen N S, Karlsen M A, Høgdall C K,etal.HE4 Tissue Expression and Serum HE4 Levels in Healthy Individuals and Patients with Benign or Malignant Tumors: A Systematic Review[J].Cancer Epidemiol Biomarkers Prev,2014,23(11):2285-2295.
[10] 陈 光,谢松元,吴 洁,等. 卵巢癌97例彩色多普勒超声与CT扫描的诊断价值比较[J]. 武警医学,2011,12(1):67-68.
[11] Shah C A, Low e K A, Paley P,etal. Influence of ovarian cancer risk status on the diagnostic performance of the serum biomarker smesothelin, HE4, and CA125[J]. Cancer Epidemiol Biomarkers Prev, 2009,18(5):1365-1372.
(2014-09-22收稿 2014-10-09修回)
(责任编辑 尤伟杰)
Serum HE4 and serum clinical significance of CA125 in diagnosis of ovarian neoplasms transvaginal color Doppler ultrasound
ZHANG Dan1,LIU Yinglan2, and LIU Xuening1.
1. Department of Ultrasonic, Heilongjiang Provincial Corps Hospital of Chinese People’s Armed Police Forces, Harbin 150076,China. 2. Department of Gynaecology and Obstetrics, First Affiliated Hospital of Harbin Medical University, Harbin 150010,China
Objective To study significance of combined with ultrasound score and serum HE4, CA125 in differentiating malignant from benign ovarian tumor. Methods Senventy-eight cases of epithelial ovarian cancer (ovarian cancer group) and 102 cases of benign ovarian tumor (benign ovarian tumor group) measured the serum level of CA125, results are expressed as median (M) said. In 80 cases of normal people as control (control group). By making the receiver operating characteristic (ROC) curve, the area under the curve (AUC) to reflect the accuracy of diagnosis. At the same time, ultrasonic scoring system scores of the two groups of patients, ultrasound scoring system and different tumor markers combination were calculated on the sensitivity, specificity of diagnosis of ovarian cancer. Results The serum HE4 and CA125 in ovarian cancer is significantly higher than that in benign ovarian tumor group and normal control group, compared the differences were statistically significant (P<0.05); Compard ovarian benign tumor group and the normal control group, HE4 showed no statistically significant difference (P>0.05), CA125 show a significant difference(P<0.05). The specificity and sensitivity of HE4 were 94.3%, 96.1%; The specificity and sensitivity of CA125 were 87.4%, 94.2%. HE4 CA125, ultrasonic scoring system of combined detection of three kinds of sensitivity of 96.1%. Conclusions HE4 and CA125 in combination with ultrasonic scoring system for differential diagnosis of the highest sensitivity.
human epididymal secretory protein; CA125; ovarian cancer; color doppler ultrasound
张 丹,硕士,主治医师,E-mail: 2206323529@qq.com
1.150076哈尔滨,武警黑龙江总队医院;2.150010,哈尔滨医科大学附属第一医院妇产科
柳英兰,E-mail: liuyinglan1975@163.com
R737.31
