Effect of Chinese Herbal Fumigation Combined with Tuina on Vertigo and Concentrations of Endothelin and Calcitonin Gene-related Peptide in Patients with Vertebral Artery Cervical Spondylosis
2014-06-27
Rehabilitation Department, Hubei Xiaogan Central Hospital, Hubei 432000, China
SPECIAL TOPIC STUDY
Effect of Chinese Herbal Fumigation Combined with Tuina on Vertigo and Concentrations of Endothelin and Calcitonin Gene-related Peptide in Patients with Vertebral Artery Cervical Spondylosis
Zhao Cheng-fei, Liu Xiao-an, Ding Yun
Rehabilitation Department, Hubei Xiaogan Central Hospital, Hubei 432000, China
Author:Zhao Cheng-fei, bachelor, resident.
E-mail: zhaochenfei_2006@126.com
Objective: To observe the effect of Chinese herbal fumigation combined with three-step tuina manipulation on concentration of endothelin (ET) and calcitonin gene-related peptide (CGRP) and vertigo in patients with vertebral artery cervical spondylosis (VACS).
Methods: A total of 120 eligible cases were randomly allocated into an observation group and a control group, 60 in each group. Cases in the observation group were treated with Chinese herbal fumigation combined with three-step tuina manipulation, whereas cases in the control group were treated with oral Flunarizine Hydrochloride Capsules.
Results: After treatment, vertigo in both groups was alleviated; there were intra-group significant differences in ET decrease and CGRP increase (P<0.01,P<0.05); and there were also inter-group significant differences (bothP<0.05).
Conclusion: Chinese herbal fumigation combined with three-step tuina manipulation can regulate the levels of ET and CGRP and improve vertigo in patients with VACS. Its therapeutic efficacy is superior to oral Flunarizine Hydrochloride Capsules.
Fumigation; Drugs, Chinese Herbal; Tuina; Massage; Spondylosis; Vertigo; Endothelins; Calcitonin Gene-related Peptide
Vertebral artery cervical spondylosis (VACS) is quite common and mainly characterized by vertebrobasilar insufficiency[1]. It often results from degeneration of the cervical spine, intraspinal and extraspinal disequilibrium and subsequent compression and irritation to the vertebral artery and nerve. Studies have shown that concentrations of endothelin (ET) and calcitonin gene-related peptide (CGRP) are correlated with sudden vertigo in VACS[2-3].
To observe the effect of Chinese herbal fumigation combined with three-step tuina manipulation on concentrations of ET and CGRP and vertigo in patients with VACS, we observed 60 cases treated in our hospital between January 2010 and May 2011, and compared with 60 cases who took oral Flunarizine Hydrochloride Capsules. The results are now summarized as follows.
1 Clinical Materials
1.1Diagnostic criteria
This is based on the diagnostic criteria for VACS proposed at the 2nd Symposium on Cervical Spondylosis in 1993[4]: typical vertigo and/or associated symptoms including nausea, tinnitus, blurred vision and sudden collapse; a history of recurrent attacks or attacks triggered by neck movement; positive Spurling sign and/or cervical rotation test; cervical X-ray suggests changes of the cervical curvature, instability or osteophyte, hyperplasia of uncovertebral joint, ligament calcification and spinal canal stenosis; transcranial Doppler (TCD) shows vertebrobasilar insufficiency on one or both sides or vertebral artery stenosis.
1.2 Inclusion criteria
1.3 Exclusion criteria
Vertigo due to cerebral arteriosclerosis, cerebellar disorders, cardiovascular disease or endocrine and metabolic problems; visual or aural vertigo; having fracture or dislocation of cervical vertebrae, cervical intervertebral disc herniation, tuberculosis, tumor and infection; aged under 18 or above 70 years; having severe diseases involving the cardiocerebrovascular, liver, kidney and hemopoietic systems; having complications of mental disorders; pregnant or breast-feeding women; those who failed to follow the treatment protocol or received other therapies or medications that can affect efficacy evaluation; those who failed to complete the course of treatment.
1.4 Statistical analysis
The SPSS 11.5 version software was used for data processing. Thet-test for measurement data, using mean ± standard deviationfor data expression, and Chi-square test for numeration data. APvalue of<0.05 indicates a statistical significance.
1.5 General data
A total of 120 VACS patients treated in our hospital between January 2010 and May 2011 were randomly allocated into two groups, 60 in each group. There were no between-group significant differences in gender, age and duration (P>0.05), indicating that the two groups were comparable (Table 1).

Table 1. Between-group comparison of general data
2 Treatment Methods
2.1 Observation group
2.1.1 Chinese herbal fumigation
Ingredients:Rou Gui(Cortex Cinnamomi),Fu Zi(Radix Aconiti Lateralis Praeparata),Chuan Xiong(Rhizoma Chuanxiong),Dan Shen(Radix et Rhizoma Salviae Miltiorrhizae),Ge Gen(Radix Puerariae Lobatae),Yin Yang Huo(Herba Epimedii),Qiang Huo(Rhizoma et Radix Notopterygii) andHong Hua(Flos Carthami).
Method: Soak 10-30 g of above ingredients into cold water for 10 min and heat them in evaporator until steam occurs. Then ask the patient to lie on the back in a multifunctional rehabilitation bed (manufactured by Xiongqing Medical Equipment Co., Ltd. of Huangshi City), and expose the neck area to the fumigation hole. With the temperature set between 40 ℃ and 55 ℃, the fumigation lasts for 30 min (Figure 1). The fumigation was done once a day, 10 times made up a course of treatment, and patients were treated for 3 courses. There was a 2-day interval between two courses.

Figure 1. Fumigation bed
2.1.2 Three-step tuina manipulation
Step 1: Relaxation by Rou-kneading and Nagrasping manipulations. With a prone position of thepatient, the practitioner applied 10-minute thumb Tui-pushing (Yi Zhi Chan), Gun-rolling, Rou-kneading and Na-grasping manipulations to patient’s nape, shoulder and upper back (Figure 2); then applied digital An-pressing or Rou-kneading to Jianjing (GB 21), Tianding (LI 17), Tianzong (SI 11) and Ashi point (Figure 3), 1 min for each point; and finally, applied Na-grasping to cervical Jiaji (EX-B 2) points, Fengchi (GB 20) and Jianjing (GB 21), 1 min for each point (Figure 4).

Figure 2. Thumb Tui-pushing manipulation

Figure 3. Digital An-pressing manipulation

Figure 4. Na-grasping manipulation
Step 2: Regulation by Bashen-pulling. With a supine position of the patient, the practitioner placed the overlapped hands over the patient’s C3, C4and C5, gently lifted the patient’s neck to pull and stretch (from top to bottom) at an angle of approximately 15° for no less than 1 min (Figure 5), using area between spinous processes as the origin of force, and repeated this for 5 times; then supported the patient’s mandible with one hand, and lifted the neck with the other hand to stretch and allow a lateral flexion of 5-8°, once to the left and once to the right (Figure 6).

Figure 5. Bashen-pulling manipulation

Figure 6. Lateral flexion manipulation
Step 3: Finish up along the meridians. With a supine position of the patient, the practitioner applied Tui-pushing (with the finger pulps of both hands) along the Governor Vessel and Bladder Meridian (from bottom to top) alternately, 5 times for each line (Figure 7); then applied parting Tui-pushing to forehead and face 5 times (Figure 8) and Na-grasping to five meridians from the anterior hairline, 5 times on the left and 5 times on the right (Figure 9); finally applied An-pressing and Roukneading to Taiyang (EX-HN 5), Yintang (GV 29), Yangbai (GB 14) and Baihui (GV 20), 1 min for each point (Figure 10).

Figure 7. Tui-pushing manipulation

Figure 8. Parting Tui-pushing manipulation

Figure 9. Na-grasping five meridians manipulation
2.2 Control group
Cases in the control group took 10 mg of oral Flunarizine Hydrochloride Capsule for each dose (before going to bed), one dose a day.
Patients in both groups were treated for three courses. Then main symptoms were scored before and after treatment.
The scoring method was shown as follows, and the therapeutic efficacy was evaluated referring to the main symptoms score.
Figure 10. An-pressing and Rou-kneading manipulations
3 Therapeutic Efficacy Observation
3.1 Observation indexes
3.1.1 Evaluation scale for cervical vertigo (ESCV)
The ESCV was adopted for scoring. The score ranges from 0 to 30. The scale consists the following 5 items.
Vertigo: 16 points including intensity of vertigo (8 points); number of attacks (4 points); and total duration of attacks (4 points).
Neck and shoulder pain: 4 points.
Headache: 2 points.
Daily living and work: 4 points.
Mental and social adaptability: 4 points.
The lower the score, the more severe the patient’s health status[5].
3.1.2 Laboratory indexes
Before treatment and after three-course treatment, 2 mL venous blood (with an empty stomach) was extracted from 7:40 am to 8:40 am. Then the blood was injected into an anti-coagulation tube containing 40 uL of aprotinin for radioimmunoassay of ET and CGRP .
3.2 Criteria for therapeutic efficacy
This is based on the therapeutic efficacy criteria for cervical spondylosis in theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[6].
Recovery: Absence of clinical signs and symptoms, normal muscle strength, normal functioning of the neck and body, and return to normal work and life.
Improvement: Alleviation of clinical signs and symptoms, relieved pain in the neck, shoulder and back and improved neck and muscle function.
Failure: Signs and symptoms remain unchanged.
3.3 Treatment results
There were no drop-out cases throughout the course of treatment. Therefore statistical analysis has been conducted on data of all patients.
3.3.1 Changes of ET and CGRP concentrations
Before treatment, there were no between-group significant differences in concentrations of ET and CGRP (bothP>0.05). After treatment, the ET concentrations in both groups were significantly decreased and CGRP concentrations in both groups were significantly increased (P<0.01,P<0.05); and there were also between-group significant differences (bothP<0.05), (Table 2).
3.3.2 Change of ESCV score
Before treatment, there was no between-group significant difference in ESVC score (P>0.05). After treatment, there were intra-group (P<0.01,P<0.05) and inter-group significant differences before and after treatment (P<0. 05), (Table 3).
3.3.3 Between-group comparison of therapeutic efficacy
After treatment, the total effective rate of the observation group was 90.0%, versus 70.0% in the control group, showing a statistical significance (P<0.05), (Table 4).
Table 2. Between-group comparison of ET and CGRP concentrations before and after treatment (, ng/L)
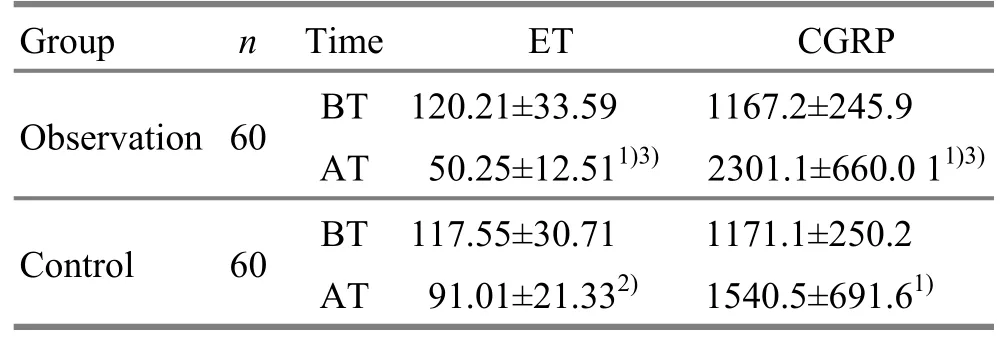
Table 2. Between-group comparison of ET and CGRP concentrations before and after treatment (, ng/L)
Note: BT=Before treatment; AT=After treatment; intra-group comparison before and after treatment, 1) P<0.01, 2) P<0. 05; compared with the control group after treatment, 3) P<0.05
?
Table 3. Between-group comparison of ESCV score before and after treatment (point)
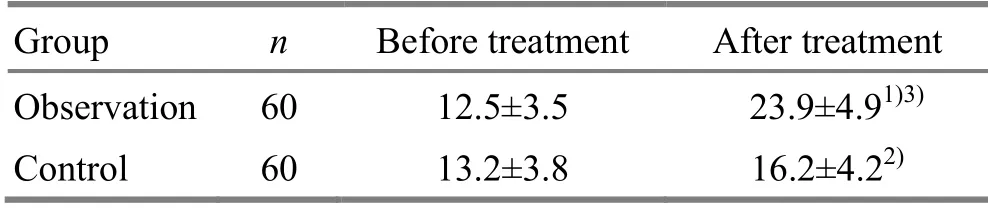
Table 3. Between-group comparison of ESCV score before and after treatment (point)
Note: Intra-group comparison before and after treatment, 1) P<0.01, 2) P<0.05; compared with the control group after treatment, 3) P<0.05
?

Table 4. Between-group comparison of therapeutic efficacy (case)
4 Discussion
VACS is a common pattern of cervical spondylosis and mainly characterized by vertebrobasilar insufficiency manifesting as sudden vertigo upon head rotation, headache, nausea, vomiting, weakness of four limbs, collapse and a history of recurrent attacks. Studies over the past years have suggested that, other than hemodynamic factors, plasma concentrations of ET and CGRP play an important role in vertebrobasilar ischemia. Endothelins are proteins that constrict blood vessels[7]and one of the major humoral factors of VACS[8]. CGRP is a potent peptide vasodilator. Plasma ET and CGRP are a pair of potent but opposed endogenous vasoconstriction and vasodilation substances. Studies have suggested that VACS patients have an elevated ET level but a decreased CGRP concentration, i.e., a vasoconstriction and vertebrobasilar insufficiency, which can in turn result in ischemia and anoxia in posterior circulation system and subsequent vertigo. As a result, the two are probably important material foundations for vertigo[9]. In terms of clinical data observation, after treatment, the ESCV scores in both groups were improved and the results were better in the observation group than that in the control group; in addition, the ET concentrations were decreased and CGRP concentrations were elevated in both groups and the results were better in the observation group than that in the control group. This indicates that Chinese herbal fumigation combined with three-step tuina manipulation can regulate meridians, circulate blood and alleviate pain in VACS patients. This method can relax cervical muscle spasm, reduce ET concentration, elevate CGRP concentration, maintain a relative balance between ET and CGRP (vasoconstriction and vasodilation). Through this, it can improve vertebral artery spasm, increase vertebral blood supply to promote local blood circulation, and improve the ischemia and anoxia in the posterior circulation and system and thus alleviate vertigo.
Of ingredients for Chinese herbal fumigation,Rou Gui(Cortex Cinnamomi) andFu Zi(Radix Aconiti Lateralis Praeparata) dissipate cold and alleviate pain;Chuan Xiong(Rhizoma Chuanxiong),Dan Shen(Radix et Rhizoma Salviae Miltiorrhizae) andHong Hua(Flos Carthami) circulate blood and resolve stasis;Yin Yang Huo(Herba Epimedii) removes wind, resolves dampness and strengthens the bones and tendons;Qiang Huo(Rhizoma et Radix Notopterygii) and (Radix Puerariae Lobatae) regulate the Bladder Meridian and Governor Vessel and lift the clean yang. The fumigation directly acts upon the affected neck area, allowing the effective ingredients to permeate into the deep affected area via the open pores. Medicinal and warm stimulation can dilate local blood vessels, increase local blood circulation, accelerate absorption of inflammation, enhance vertebral blood supply, relax local muscle spasm, alleviate compression to the cervical intervertebral disc and thus relieve compression or torsion of degenerative changes to vertebral artery. On one hand, Chinese herbal fumigation combined with three-step tuina manipulation can target the root cause. On the other hand, it can relax local muscle spasm and soft tissue injury, relieve irritation and compression to the nerves and blood vessels, restore stability between bones and joints, increase local blood circulation and vertebral blood supply and thus alleviate vertigo and restore normal physiology of the cervical vertebrae[10-12]. In short, this is a safe, simple, effective and economical therapy for VACS patients and worthy of further clinical application.
Conflict of Interest
The authors declared that there was no potential conflict of interest.
Acknowledgments
This work was supported by Hubei Xiaogan Central Hospital.
Statement of Informed Consent
All of the patients in the study signed the informed consent.
[1] Sun HW, He JL, Li YW, Chen YQ. Correlation between cervical spondylosis and blood rheology. Zhongyi Zhenggu, 1993, 5 (3): 7-9.
[2] Dai YH, Cheng GH, Su XL. Changes of plasma concentrations of vasoactive factors in early canine arteriostenosis. Fangshe Mianyi Zazhi, 2007, 20(1): 7-9.
[3] Wang LL, Liu XY. Clinical significance of plasma concentrations of ET, CGBP and NSE in patients with vertebrobasilar insufficiency. Fangshe Mianyi Zazhi, 2007, 20(3): 212-214.
[4] Sun Y, Chen FQ. Summary of the 2nd symposium on cervical spondylosis. Zhonghua Waike Zazhi, 1993, 31(8): 472-476.
[5] Zhuo DH. Rehabilitation Medicine in China. 2nd Edition. Beijing: Huaxia Publishing House, 2003: 1148.
[6] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1994: 186.
[7] Dong HJ, Xu PX. The research progress of endothelin axis. Wujing Yixueyuan Xuebao, 2009, 18(6): 557-560.
[8] Li CN, Yang MX. Etiology, pathogenesis and treatment advance in vertebral artery-related cervical spondylosis. Zhongyi Zhenggu, 2008, 20 (2): 66-68.
[9] Wei JJ, Zhang JJ, Ciao JS. Clinical significance of plasma concentrations of ET and CGBP in patients with cervical vertigo. Cuzhong Yu Shenjing Jibing, 2005, 12 (1): 38-39.
[10] Li XM. Tuina plus traction for 120 cases with vertebral artery-related cervical spondylosis. Huaihai Yiyao, 2001, 19(6): 486.
[11] Yue FL, Liang SD, Zhu YW, Zhao CY, Chen Y, Li YF, Zhang YZ. Clinical study on massage in treating cervical spondylosis of vertebral artery type. J Acupunct Tuina Sci, 2011, 9(3): 188-192.
[12] Cheng SD, Luo JS, Lu NZ, Zhang TW, Hu ZJ, Pu JS, Li W, Xu HL, Wang HF, Huang J. A randomized controlled trial of warm needling moxibustion plus sitting-position pulling and stretching manipulation for the treatment of cervical spondylotic vertebral arteriopathy. Shanghai Zhenjiu Zazhi, 2012, 31(6): 410-413.
Translator:Han Chou-ping
Received Date:July 15, 2014
R244.1
: A
met the above criteria;
no treatment 2 weeks prior to the clinical trial; aged between 18 and 70 years; those who were willing to sign the informed consent and cooperate throughout the required course of treatment.
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Warm Needling Moxibustion at Zhongji (CV 3) and Zusanli (ST 36) for Urinary Retention after Gynecological Surgery
- Therapeutic Efficacy Observation on Acupoint Sticking for Edema Due to Chronic Cardiac Failure
- Therapeutic Efficacy Analysis of Balancing Yin-yang Manipulation for Post-stroke Upper Limb Spasticity
- Acupoint Massage in Relieving Pain after Ureteroscopic Holmium Laser Lithotripsy
- Tuina plus Ultrasonic Therapy for Infantile Muscular Torticollis
- Personal Experience on Palpation of the Spine