Clinical Study on Tuina Combined with Auricular Point Sticking for Cervical Radiculopathy
2014-06-19
Tuina Department, Longhua Hospital, Shanghai University of Traditional
Chinese Medicine, Shanghai 200032, China
CLINICAL STUDY
Clinical Study on Tuina Combined with Auricular Point Sticking for Cervical Radiculopathy
Wang Sai-na, Sheng Feng, Pan Yun-hua, Xu Feng, Wang Zhi-chao, Cheng Lei
Tuina Department, Longhua Hospital, Shanghai University of Traditional
Chinese Medicine, Shanghai 200032, China
Objective: To observe the clinical effect of tuina combined with auricular point sticking on cervical radiculopathy and evaluate in health economics.
Methods: Using randomized single-blind controlled clinical design, a total of 72 cases with cervical radiculopathy were randomly allocated into an observation group or a control group by the ratio of 1:1, 36 in each group. Cases in the observation group were treated with tuina combined with auricular point sticking, whereas cases in the control group were treated with tuina alone. Then the clinical effects in the two groups were observed and the cost of health economics was evaluated.
Results: The drop-out, recovery, improvement and failure cases, recovery rate and total effective rate in the observation group were 1, 15, 20, 0, 42.9% and 100% respectively, versus 2, 6, 23, 5, 17.6% and 85.3% in the control group, showing significant differences in recovery rate and total effective rate (P<0.05). As for health economics, the cost-effect in the observation group was better than that in the control group.
Conclusion: Compared with tuina alone, tuina combined with auricular point sticking can obtain better effect and lower cost in health economics for cervical radiculopathy.
Tuina; Massage; Auricular Point Sticking; Spondylosis; Neck Pain; Acupressure; Health Care Economics and Organizations
Cervical spondylosis (CS) is a very common disorder. As an important conservative therapy for CS, tuina can effectively control its symptoms and direct at the etiological factors. In addition, it does not cause adverse reactions[1]. When used in combination with tuina, auricular point sticking plus self-massage can increase the treatment effect for CS and decrease the cost in health economics. We treated cervical radiculopathy patients with tuina combined with auricular point sticking between April 2013 and March 2014, and observed its clinical effect and evaluated cost-effect in health economics. The results are now summarized as follows.
Author: Wang Sai-na, master of
medicine, attending physician
1 Clinical Materials
1.1 Diagnostic criteria
This was based on the criteria stipulated in the Second Symposium on Cervical Spondylosis held in Qingdao in October 1992[2]: typical radicular symptoms (numbness, pain) in the area where the nerve that is irritated travels; decreased skin sensation innervated by the compressed nerve root, abnormal tendon reflex, muscle atrophy and decreased muscle strength;positive brachial plexus tension test and crushing test of intervertebral foramen; hyperplasia of the vertebrae and uncovertebral joints and narrowing of intervertebral spaces confirmed by cervical X-ray examination; and exclusion of those who mainly presented with pain on the upper limb due to other conditions (such as thoracic outlet syndrome, tennis elbow, carpal-tunnel syndrome and scapulohumeral periarthritis).
1.2 Inclusion criteria
Those who met the above diagnostic criteria; men and women aged between 30-65 years old; having no problems involving the spinal cord or central nervous system; having agreed not to accept other therapies during this study (including oral or external muscle relaxant); those who were willing to participate in this study and sign the informed consent.
1.3 Exclusion criteria
Those who met the above criteria but had other patterns of cervical spondylosis; having complications of hypertension, heart disease, arteriosclerosis, anemia and severe osteoporosis; having suspected or confirmed tumor in the neck, spinal canal or brain; having disorders involving the spinal cord and central nervous system, manifesting muscle tone changes (such as stroke, sequelae of stroke, syringomyelia and muscular dystrophy); having taken other therapies that may affect efficacy evaluation; having severe skin lesion or skin diseases that are not suitable for tuina treatment; those who were reluctant to participate in this study.
1.4 Rejection, dropout and termination criteria
1.4.1 Rejection criteria
The following subjects will be rejected: those who failed to meet the inclusion criteria but were recruited by mistake; those who met the inclusion criteria but didn’t receive treatment after being recruited.
1.4.2 Dropout criteria
The following subjects will be considered drop-out: those who didn’t complete the trial and left halfway or drop out assumed by doctors; those who failed to stick to the treatment protocol or received other therapies or medications that may interfere with efficacy evaluation.
1.4.3 Termination criteria
The following subjects will be terminated: those who cannot continue with treatment because of complications, severe adverse reactions or special physiological changes; major issues in the design or test that may interfere with therapeutic efficacy evaluation.
1.5 Statistical method
The Microsoft Excel 2003 database and SPSS 16.0 version software were used for data analysis. The measurement data were expressed byThet-test or Mann-WhitneyUtest was used to compare changes between before and after treatment. The numeration data were expressed by absolute frequency (constituent ratio) and Chi-square test or nonparametric test was used for changes between before and after treatment.
Effectiveness analysis: The therapeutic efficacy in two groups was analyzed by rank sum test.
Safety analysis: The incidences of adverse reactions in two groups were compared by Chi-square test and adverse events during this trial were listed. This study also analyzed the changes of laboratory results and their relationships with intervention factors. APvalue of less than 0.05 indicated a statistical significance.
1.6 General data
A total of 72 cervical radiculopathy cases were outpatients treated in the Tuina Department, Longhua Hospital, Shanghai University of Traditional Chinese Medicine. They were randomly allocated into an observation group or a control group, 36 in each group. There were no significant differences in gender, age, duration and disease severity between two groups (two-sided test,P>0.05), indicating that the two groups were comparable (Table 1).
Three cases (4.2%) dropped out during the study, including 1 case from the observation group and 2 cases form the control group. A total of 69 cases met the criteria for therapeutic efficacy analysis. Please see Figure 1 for the clinical flow chart of the patients in the two groups.

Table 1. Between-group comparison of baseline materials
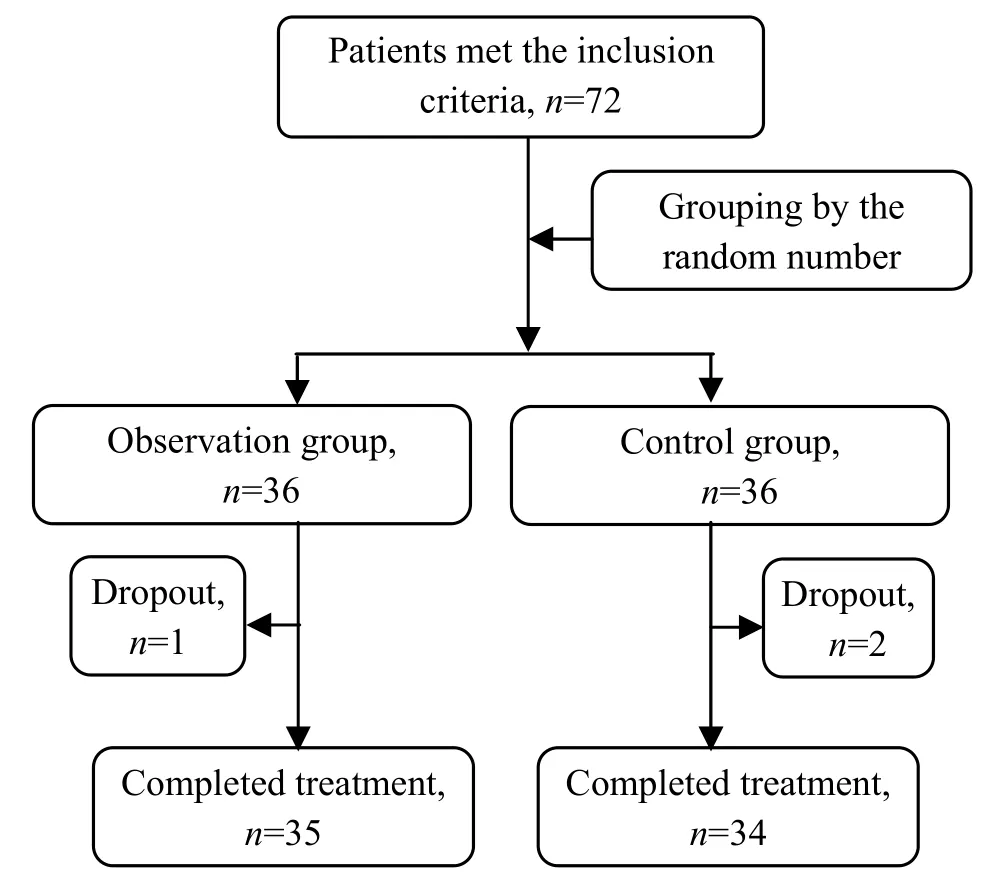
Figure 1. Clinical flow chart of the two groups
2 Research Methods
Randomized single-blind controlled clinical trial was designed for this study. The sample size was estimated according to the superiority clinical trial sample size formula[3]:n=(Uα+U1-β)×[P1×(1-P1)+P0×(1-P0)]÷(P1-P0).
The case numbers were arranged by equal proportion, and superiority one-sided test was employed.α=0.05, β=0.2 (effectiveness=80%). The estimated effective rate in the observation group P1=0.90 (90%), versus P0=0.7 (70%) in the control group, and the superiority standard was 0.23. Based on estimation, there should be 30 cases in each group. Considering a 20% dropout rate, a total of 72 cases were recruited, 36 in each group.
2.1 Observation group
2.1.1 Tuina treatment
The method and procedure were based on the 5th edition ofScience of Tuina. Rou-kneading, Gun-rolling, Na-grasping and Cuo-twisting methods were used in this study.
Major acupoints: Fengchi (GB 20), Jianjing (GB 21), Jianwaishu (SI 14), Jianyu (LI 15), Quchi (LI 11), Shousanli (LI 10) and Hegu (LI 4).
Method: The patient took a sitting position. First, apply 3-minute Rou-kneading to Fengchi (GB 20), Jianjing (GB 21), Jianwaishu (SI 14), Jianyu (LI 15), Shousanli (LI 10) and Hegu (LI 4); then stand behind the patient and apply 10-minute Gun-rolling to the shoulder, using the force of 4 kg and frequency of 120 times per minute; finally, apply 3 times of Na-grasping to the back of neck and bilateral Jianjing (GB 21). The treatment was done once every other day, 3 times a week and 10 times constituted a course of treatment. The therapeutic efficacy was observed after one course of treatment.
2.1.2 Auricular point sticking
The magnetic ear seeds manufactured by Suzhou Medical Appliance Factory Co., Ltd. were used in this study. Practitioners were trained on auricular point sticking before treatment.
Major points[4]: Cervical Vertebrae (AH13), Liver (CO12), kidney (CO10), Shenmen (TF4) and Subcortex (AT4).
Adjunct points: Positive reaction points within the scapha.
Method: Immobilize the auricle using the left hand and identify the sensitive points using a probe in the right hand. Then press the points and leave pressure marks. After sterilization using 75% alcohol, stick the magnetic seeds to the pressure marks and press for seconds until occurrence of warm, sore, distending or radiating sensations (within the patient’s pain tolerance). The magnetic seeds were used for two ears alternately and exchanged once every other day. The patients were asked to press 2-3 times a day, 3-5 min each time until the occurrence of sore, distending, warm or radiating sensation. The treatment was done 3 times a week and 10 times constituted a course of treatment. Patients may need a referral if they did not respond after 10 times of treatments.
2.2 Control group
Same tuina treatment (same method, points and course of treatment) as that in the observation group was used in the control group.
3 Treatment Result Observation
3.1 Observation indexes
3.1.1 Assessment scale for cervical spondylosis[2]
The Assessment Scale for Cervical Spondylosis stipulated by the Rehabilitation Center, Huaxi Hospital Affiliated to Sichuan University was used before and after treatment to evaluate the functions of the cervical vertebrae.
The scale consists of three items: subjective symptoms, clinical examination and daily living. Patients were asked to fill in each item. The improvement index and/or improvement rate were then calculated according to the scores before and after treatment.
下面,笔者就从这几个方面,结合教学实践,简单进行论述,以期同大家一起分享和交流高中数学有效课堂构建的问题,以促进数学课堂的有效性的落实.
Subjective symptoms (highest point: 10) including pain in the neck, shoulder and back (5 grades: 0-4 points), pain and/or numbness in upper limbs (5 grades: 0-4 points) and headache and vertigo (3 grades: 0-2 points).
Clinical examination (highest point: 21) including tenderness (4 grades: 0-9 points), pressing test of vertex and/or crushing test of intervertebral foramen,brachial plexus tension test and neck extension test (negative: 2 points; positive: 0), tendon reflex (normal: 2 points; weakened: 1; absence: 0), sensory disturbance or paresthesia (3 grades: 0-2 points) and muscle strength grading (0-V: 0-2 points).
Daily living (highest point: 4) including neck movement (3 grades of flexion, extension and rotation: 0-2 points) and weight-bearing of the affected limb (3 grades: 0-2 points).
The total score of the assessment scale is 35 points. The lower the score, the severer the condition.
3.1.2 Superficial cervical muscle pain assessment
The simplified McGill pain questionnaire (MPQ) was used to evaluate superficial cervical muscle pain. The self-report questionnaire was filled before and after treatment according to the patients’ subjective feeling.
The scale comprised of a straight line marked from 0 to 10, including 10 equal parts. One end was marked ‘no pain’ and the other end ‘intense pain’. The patients were asked to mark their pain intensity in the corresponding position. Then assessment was made by doctors (from 0 to 10 points).
3.1.3 Health economics evaluation
Clinical economics in the two groups were then evaluated and compared, i.e., the cost-effect ratios in the two groups were calculated[5-6]. The effect was expressed using clinical effective rate.
Cost-effect ratio=Total cost ÷ Clinical effective rate.
3.2 Therapeutic efficacy criteria[7]
The improvement was calculated according to the assessment score before and after treatment.
Improvement index=(Pre-treatment score — Posttreatment score) ÷ Post-treatment score.
The therapeutic efficacy criteria were then made according to the improvement index and alleviation of clinical symptoms.
Recovery: In absence or almost in absence of signs and symptom, the improvement index ≥95%.
Improvement: Alleviated signs and symptoms, improvement index ≥30% but <95%.
Failure: Signs and symptoms remained unchanged, improvement index <30%.
3.3 Treatment results
3.3.1 Between-group comparison of clinical effects
After treatment, there were significant differences in recovery rate and total effective rate between the two groups (P<0.05), indicating a better effect in the observation group than that in the control group (Table 2).
3.3.2 Between-group comparison of health economics
There was no statistical significance in comparing the total cost between the two groups (P>0.05). There was a statistical significance in comparing the cost-effect ratio between the two groups (P<0.05). This indicates that although the total amount in the two groups was similar but the cost-effectiveness was better in the observation group than that in the control group (Table 3).
3.3.3 Drop-out cases and compliance of the patients
A total of 3 cases, including 1 case in the observation group and 2 cases in the control group, dropped out in this study. There was no significant difference between the two groups (P>0.05), indicating a content compliance of the patients in both groups.

Table 2. Between-group comparison of clinical effects (case)
Table 3. Between-group comparison on cost-effectiveness

Table 3. Between-group comparison on cost-effectiveness
Note: Compared with the control group, 1) P<0.05
?
3.3.4 Safety evaluation
No adverse reactions (such as skin lesion, soft tissue injury, bone/joint injury or aggravated pain) or major events (such as faint) occurred during the treatment.
4 Discussion
Cervical spondylosis is a very common disorder and cervical radiculopathy is one of the most common patterns. The incidence of CS tends to increase year by year because of lifestyle changes and work or life stress. It’s clinically characterized by pain and numbness of the neck and arm as well as restricted movement of the neck. These symptoms can greatly affect people’s life and work.
This condition is caused by chronic degenerative changes of the intervertebral disc. These changes, coupled with strain or trauma, can result in dynamic and static instability of the cervical spine, subsequently leading to herniated cervical disc, intervertebral joint subluxation and bone spurs on either cervical facet or uncovertebral joint. This can further compress one or more of the nerve roots, causing a series of symptoms (pain in the neck, shoulder and back and pain/numbness in the upper limb). Tuina can circulate qi, invigorate blood, relax adhesion and correct the subluxation. By stimulating the receptor of local points and inhibiting the excitability of sympathetic nerve, tuina manipulation can increase local blood circulation, relax muscle and vascular spasm, promote absorption of inflammatory pain-related substance, relieve mechanical compression and immunological irritation to nerve roots, correct intervertebral joint subluxation, restore dynamic and static balance of the cervical spine and thus alleviate clinical symptoms[8-12].
Ears are the gathering places of meridians. Of the twelve regular meridians, the Gallbladder, Triple Energizer and Small Intestine Meridians directly enter the ears; the Stomach and Bladder Meridians are close to the ears. Through the connection of meridians, ears are associated with the entire body. As for meridians in the cervical area, the Bladder, Triple Energizer, Gallbladder Meridians and the Governor Vessel are especially associated with cervical spondylosis. Pressing ear points the Cervical Vertebrae (AH13), Liver (CO12), Kidney (CO10), Shenmen (TF4) and Subcortex (AT4) can alleviate pain, regulate meridian qi and blood, restore yin-yang balance and thus alleviate neck stiffness[13-16].
This study has proven that tuina combined with auricular point sticking is safe and reliable for cervical radiculopathy. In addition, it is superior to tuina alone in improving symptoms, daily living, self-satisfaction and local muscle pain.
Health economics is a branch of economics concerned with issues related to efficiency, effectiveness, value and behavior in the production and consumption of health and health care. We intended to investigate the value of tuina combined with auricular point sticking in health economics and provide decision-making evidence. As one of the most common approaches in health economics evaluation[17], cost-effectiveness analysis can help us find a treatment protocol with minimal cost, i.e., an optimal balance point between cost and effect. Judging from this study, the total cost of two treatment methods were similar; however, tuina combined with auricular point sticking obtained a better cost-effect ratio than tuina alone. This study enriched the clinical therapeutics in Chinese medicine and laid a solid foundation for multi-center and large sample clinical trial in the future.
Conflict of Interest
The authors declared that there was no conflict of interest in this article.
Acknowledgments
This work was supported by Project of Longhua Hospital, Shanghai University of Traditional Chinese Medicine (No. 2013YM09); the Ding’s Tuina Project, Three-year Plan of Shanghai Traditional Chinese Medicine Development (Inheritance Project for Shanghai Schools of Traditional Chinese Medicine) (No. ZYSNXD-CC- HPGC-JD-011).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.
[1] Li PG, Wu Z, Luo J, Sun SC. Summary on nerve root cervical spondylopathy treated with Chinese medicine. Zhongyiyao Xinxi, 2005, 22(5): 19-21.
[2] Wang XH, He CQ, Ding MP, Zhang LM, Han M, Zhang YM, Lan Q. Assessment scale for cervical spondylosis. Huaxi Yixue, 2005, 20(2): 232-233.
[3] Jin PH. Statistical Methods in Medicine. 2nd Edition. Shanghai: Fudan University Press, 2003: 469-473.
[4] Yang GR, Zhang JW. Clinical observation on auricular point sticking for vertebral artery type of cervical spondylosis in 50 cases. Hebei Zhongyi, 2007, 29(7): 623-624.
[5] Zhang N, Shi XF, Wu J. The application of incremental cost-effectiveness ratio to health technology assessment. Zhongguo Weisheng Zhengce Yanjiu, 2012, 5(2): 64-68.
[6] Bambha K, Kim WR. Cost-effectiveness analysis and incremental cost-effectiveness ratios: uses and pitfalls. Eur J Gastroenterol Hepatol, 2004, 16(6): 519-526.
[7] Ministry of Health of the People’s Republic of China. Guiding Principles for Clinical Study of New ChineseMedicines. Beijing: China Medico-Pharmaceutical Science & Technology Publishing House, 2002: 346-349.
[8] Zhou JW, Hu LX, Li N, Zhang F, Li CY, Zhao JJ, Li J, Hu YG, Zhang Y, Wang CW. Multicenter randomized controlled study on acupuncture-massage comprehensive program for treatment of cervical spondylosis of arterial type. Zhongguo Zhenjiu, 2005, 25(4): 227-231.
[9] Lu JZ, Li YP. Clinical observation on electroacupuncture plus sitting-position pulling and stretching reduction manipulation for the treatment of cervical vertigo. Shanghai Zhenjiu Zazhi, 2013, 32(6): 495-496.
[10] Hua Y. Clinical observation on treatment of cervical spondylotic radiculopathy with combined electroacupuncture tuina and traction. J Acupunct Tuina Sci, 2009, 7(3): 156-158.
[11] Peng ZL, Huang J. Observations on the efficacy of acupuncture plus massotherapy in treating vertebroarterial cervical spondylopathy. Shanghai Zhenjiu Zazhi, 2009, 28(1): 29-30.
[12] Ni CC, Yao LM, Shen ZF, Yan YQ. Therapeutic efficacy observation on combining intermittent traction with warm needling for cervical radiculopathy. J Acupunct Tuina Sci, 2013, 11(6): 367-370.
[13] Jia CS, Ma XS, Ge JJ. Preliminary clinical observation on rapid analgesia effect of otopuncture point penetration method in treating cervical spondylopathy. Zhongguo Zhongyiyao Xinxi Zazhi, 2002, 9(10): 56-57.
[14] Zhang H, Qian LL. Observations on the immediate effect of ear-acupuncture combined treatment on cervical vertigo. Shanghai Zhenjiu Zazhi, 2009, 28(11): 643-644.
[15] Yue JH, Zhang QH, Wang SL, Gao WB. Research progress of electroacupuncture treatment on cervical spondylosis radiculopathy in recent ten years. J Acupunct Tuina Sci, 2011, 9(2): 127-132.
[16] Yuan X. Observations on the curative effect of auricular plaster therapy on vertebral artery-type cervical spondylopathy. Shanghai Zhenjiu Zazhi, 2007, 26(8): 13-14. [17] Cheng XM. Health Economics (for the Major of Preventive Medicine). Beijing: People’s Medical Publishing House, 2012: 551.
Translator: Han Chou-ping
R244.1
: A
Sheng Feng, master of medicine, associate chief physician.
E-mail: saina1234@126.com
Date: April 20, 2014
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Observation on the Effect of Acupoint Injection plus Massage Therapy on Primary Dysmenorrhea
- Observation on Warm Needling Therapy for Third Lumbar Vertebra Transverse Process Syndrome
- Clinical Observation on Comprehensive Treatment on Cutaneous Region for Low Back Pain
- Tuina for Leg Length Discrepancy and Lumbosacral Pain Due to Sacroiliac Joint Subluxation
- Clinical Observation on Acupuncture Combined with Hyperbaric Oxygenation in Treating Patients with Cervical Spondylosis of Nerve Root Type in Acute Phase
- Clinical Study on Acupoint Injection plus Acupuncture for Insomnia Due to Heart-kidney Disharmony