老年临终期肿瘤患者合并肺部感染的危险因素分析
2014-04-23姜宏宁张慧荣龙霖梓
杨 波,姜宏宁,余 敏,张慧荣,龙霖梓
老年临终期肿瘤患者合并肺部感染的危险因素分析
杨 波*,姜宏宁,余 敏,张慧荣,龙霖梓
(北京老年医院关怀病房,北京 100095)
分析老年临终期恶性肿瘤患者肺部感染的发生情况及其危险因素。回顾性地分析2012年10月至2013年11月期间在北京老年医院住院治疗的143例老年临终期恶性肿瘤患者的临床资料,采用多因素logistic回归分析方法对87例并发肺部感染病例(观察组)及56例未并发肺部感染病例(对照组)进行比较分析。logistic多因素逐步回归分析显示,肺癌[比值比(OR)=4.137,95%置信区间(CI)为1.967~14.479]、意识障碍(OR=3.728,95%CI为1.313~8.315)、低蛋白血症(OR=2.960,95%CI为1.300~6.739)、住院天数(OR=2.611,95%CI为1.056~6.451)、体力状况(OR=2.187,95%CI为1.345~4.071)、糖尿病(OR=1.937,95%CI为1.159~3.238)、慢性阻塞性肺疾病(OR=1.823,95%CI为1.056~3.891)与老年临终期恶性肿瘤患者并发肺部感染有相关性(均<0.05)。肺部感染是老年临终期恶性肿瘤患者的常见并发症,肺癌、伴有意识障碍、低蛋白血症、住院时间长、卧床以及合并慢性基础病(糖尿病和慢性阻塞性肺疾病)者是老年临终肿瘤患者并发肺部感染的危险。
老年人;恶性肿瘤;肺部感染;危险因素;临终关怀医疗
临终患者指处于各种疾病终末阶段、预计生存期<6个月的患者,其中恶性肿瘤患者占大多数[1]。伴随我国社会人口老龄化和恶性肿瘤的高发病率,以及肿瘤患者对自身生活质量的重视,老年临终期恶性肿瘤患者的就诊率逐渐增加。老年临终期肿瘤患者由于脏器功能衰退、肿瘤导致的免疫力降低,以及合并慢性基础疾病等因素,易合并感染。在对实体瘤死者进行尸体解剖后发现,47%的患者死于感染[2]。在各种感染中,肺部是最常见的感染部位之一,且死亡率高,对患者生活质量影响显著[3]。为探讨老年临终期恶性肿瘤患者并发肺部感染的相关危险因素,比较研究我院143例老年临终期恶性肿瘤患者的临床资料,分析报告如下。
1 对象与方法
1.1 研究对象
选择2012年10月至2013年11月期间在北京老年医院住院治疗的老年临终期恶性肿瘤患者,入选标准:(1)年龄≥60岁;(2)肿瘤分期:根据国际抗癌联盟(Union for International Cancer Control,UICC)TNM分期为Ⅳ期;(3)预计生存期<6个月。排除标准:(1)血液系统恶性肿瘤;(2)放、化疗后免疫及造血功能抑制期。肺部感染的诊断符合中华医学会呼吸病学会制定的诊断标准[4,5]。
1.2 研究方法
回顾性地分析入组患者的病历记录,制定统一调查表。内容包括可能与肺部感染相关的13个因素:性别、年龄、伴随疾病[慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)、糖尿病]、吸烟史、住院天数、肿瘤原发部位、体力状况评分(评分项目称为肿瘤学东方合作组工作状态,Eastern Cooperative Oncology Groups Performance Status,ECOG)、意识状态、实验室检查结果(包括血红蛋白、白蛋白水平)、糖皮质激素应用、侵入性操作。
1.3 统计学处理
2 结 果
2.1 老年临终期恶性肿瘤患者并发肺部感染的单因素分析
本组143例患者中并发肺部感染者56例(39.16%),年龄61~87(70.36±6.39)岁,男30例(53.57%),女26例(46.43%)。未并发肺部感染者87例(60.84%),年龄60~82(68.24±5.33)岁,男42例(48.28%),女45例(51.72%)。单因素分析中,年龄、COPD、糖尿病、吸烟史、住院天数、肿瘤原发部位、体力状况评分、意识状态、白蛋白水平、侵入性操作差异有统计学意义(<0.05);性别、血红蛋白水平、糖皮质激素应用组间比较,差异无统计学意义(>0.05;表1)。
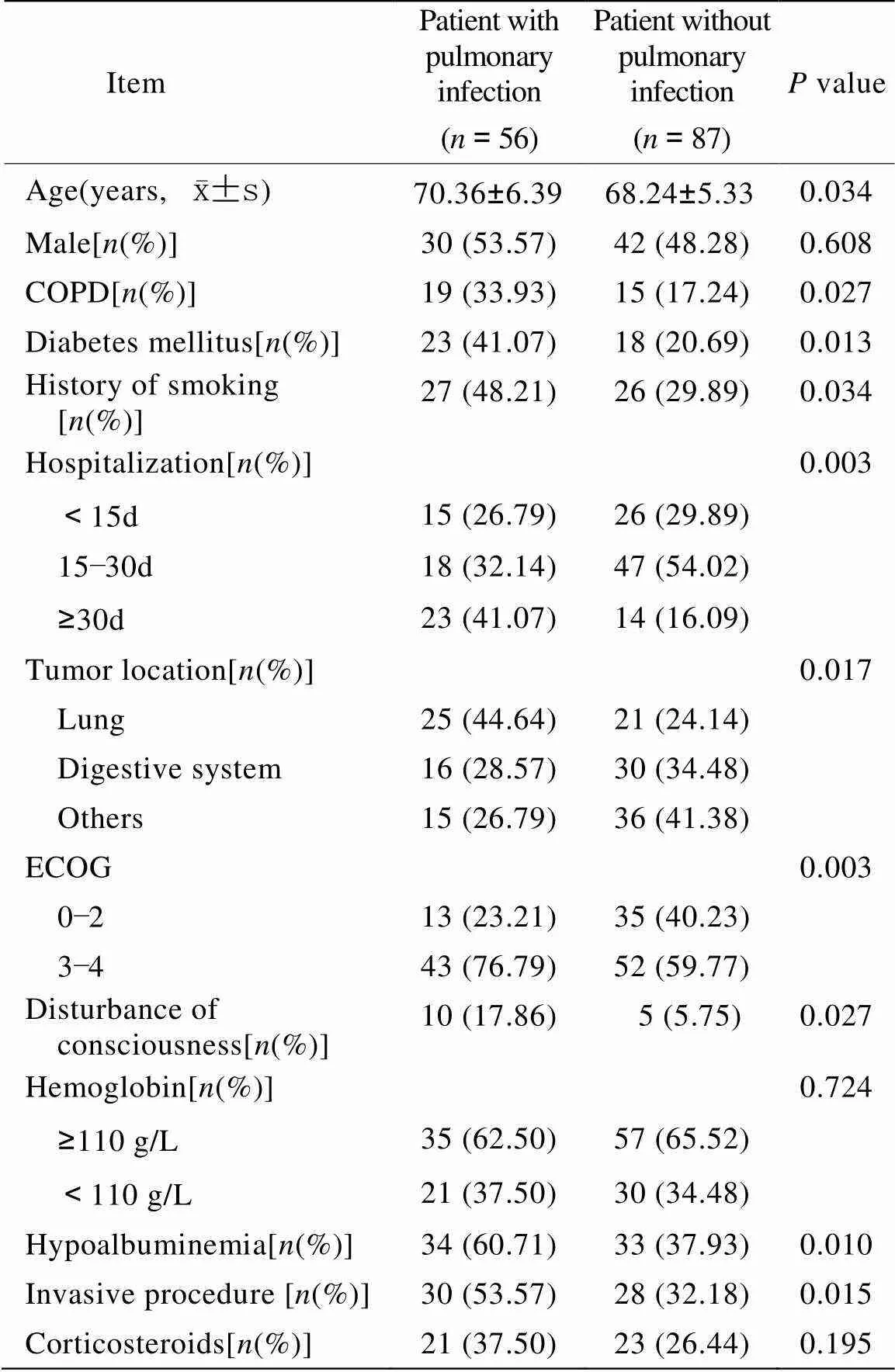
表1 两组患者的临床情况对比
COPD: chronic obstructive pulmonary disease; ECOG: Eastern Cooperative Oncology Groups Performance Status
2.2 老年临终期恶性肿瘤患者并发肺部感染的多因素分析
将单因素分析中<0.1的变量进一步纳入多因素非条件logistic逐步回归分析,各变量代表因素及赋值见表2。结果显示,老年临终期恶性肿瘤患者并发肺部感染的危险因素(按OR值从高至低排序)是,肺癌、意识障碍、低蛋白血症、住院天数、体力状况评分、糖尿病、COPD(表3)。
3 讨 论
本研究表明,肺部感染是老年临终期恶性肿瘤患者的常见并发症,发生率达39.16%,与国内外其他研究结果类似(27%~42%)[6−8]。研究结果显示,肿瘤原发部位、意识障碍、低蛋白血症、住院天数、体力状况评分、糖尿病、COPD是老年临终期肿瘤患者并发肺部感染的危险因素。
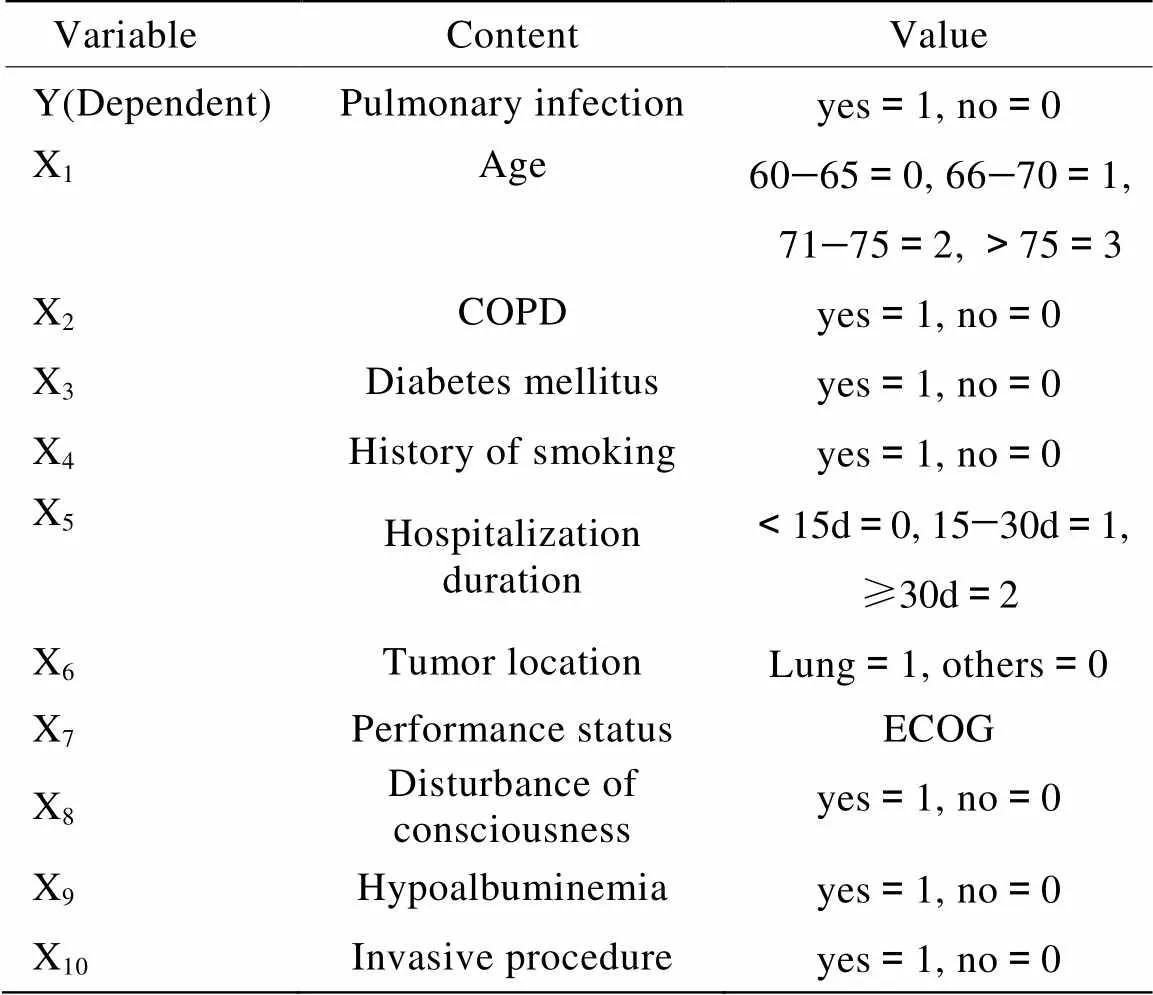
表2 Logistic回归分析变量赋值表
COPD: chronic obstructive pulmonary disease
老年临终期肿瘤患者的以下特点决定其肺部感染的高发生率:(1)患者处于恶性肿瘤终末阶段,肿瘤的消耗导致机体免疫功能降低,增加感染机会;(2)随年龄增加,机体的脏器功能逐渐退化,且老年患者常常合并导致机体抵抗力下降的一种或多种慢性疾病,如糖尿病、慢性呼吸系统疾病等;(3)临终期患者病情重,住院时间长,增加院内感染的机会;(4)老年临终期患者体力状况下降,身体活动减少,卧床时间延长,肺部感染概率明显增加;(5)老年临终期患者咳嗽反射减弱,支气管黏膜纤毛运动减弱,易使口咽部的条件致病菌向下呼吸道蔓延,发生支气管及肺部感染;(6)合并意识障碍者自身防御反射减弱,呼吸道分泌物不能及时清除,同时患者多伴有吞咽功能异常,易发生误吸[9]。
与其他部位的肿瘤患者相比,终末期肺癌患者并发肺部感染的发生率更高。原因在于,肺癌破坏呼吸系统的防御功能;肿瘤分泌免疫抑制因子,抑制机体的抗肿瘤免疫功能[10];肿瘤直接浸润气管、支气管、肺泡等,导致呼吸系统分泌物增多,如痰液引流不畅,极易诱发感染;肿块阻塞支气管直接造成远段肺组织继发感染[11]。
本组老年临终期肿瘤患者中,合并肺部感染者的年龄大于非肺部感染者(<0.05),然而进一步logistic回归分析发现,年龄不是老年临终期肿瘤患者的独立危险因素。Williams等[12]在其研究中发现,肿瘤患者的感染发生率与年龄无关。糖皮质激素是晚期肿瘤患者的常用药物之一,对于改善临终期患者的呼吸困难、疼痛等常见症状有明确的作用[13]。本组患者中,糖皮质激素的应用并未导致肺部感染的增加。这一结果与Reinbolt等[14]对1 731例晚期肿瘤患者的前瞻性试验结果一致。
尽管感染是晚期肿瘤患者的最常见死因[7],临终期肿瘤合并感染患者的治疗却仍存在争议,目前缺乏统一的治疗指南[3]。一方面,有研究发现抗感染治疗能够延长临终期患者的生存时间,提高生活质量[2,15];另一方面,Oneschuk等[16]认为对于生存期<1周的临终患者,抗感染治疗不能获益。此外,部分学者认为,对于临终期患者进行抗感染治疗,应把控制症状作为主要目标,而非延长生存期[14,17−19]。
综上所述,肺部感染是老年临终期恶性肿瘤患者的常见并发症。重视对患者进行危险分层,对高危患者密切监测,加强对感染的预防。对于合并肺部感染者,结合患者的预后、患者和家属的治疗目标、患者的整体状况等,权衡抗感染治疗的获益和可能带来的不良反应,给予个体化治疗,以提高临终期肿瘤患者的生活质量。
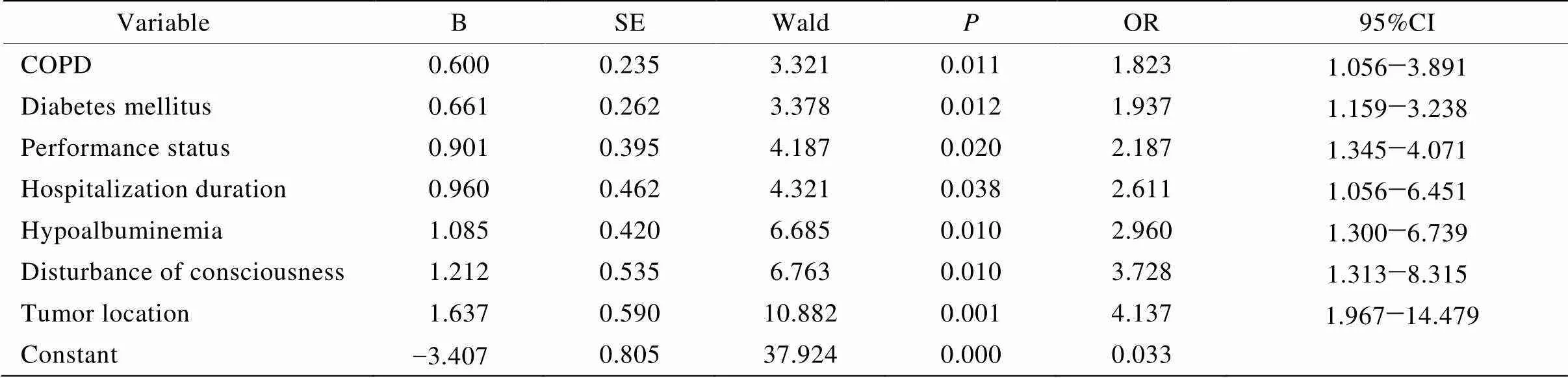
表3 老年临终肿瘤患者并发肺部感染的多因素logistic回归分析结果
COPD: chronic obstructive pulmonary disease
[1] Meng XW. Hospice Care[M]. Tianjin: Tianjin Science and Technology Press,2002: 1−2 [孟宪武. 临终关怀[M]. 天津: 天津科学技术出版社, 2002: 1−2.]
[2] Thai V, Lau F, Wolch G,. Impact of infections on the survival of hospitalized advanced cancer patients[J]. J Pain Symptom Manage, 2012, 43(3): 549−557.
[3] Nagy-Agren S, Haley HB. Management of infections in palliative care patients with advanced cancer[J]. J Pain Symptom Manage, 2002, 24(1): 64−70.
[4] Chinese Society of Respiratory Diseases. Guidelines for the Diagnosis and Treatment of Hospital-acquired Pneumonia(Draft)[J]. Chin J Tuberc Respir Dis, 1999, 22(4): 201−203. [中华医学会呼吸病学分会. 医院获得性肺炎诊断和治疗指南(草案)[J]. 中华结核和呼吸杂志, 1999, 22(4): 201−203.]
[5] Chinese Society of Respiratory Diseases. Guidelines for the Diagnosis and Treatment of Community-acquired Pneumonia[J]. Chin J Tuberc Respir Dis, 2006, 29(10): 651−655. [中华医学会呼吸病学分会. 社区获得性肺炎诊断和治疗指南[J]. 中华结核和呼吸杂志, 2006, 29(10): 651−655. ]
[6] Pereira J, Watanabe S, Wolch G. A retrospective review of the frequency of infections and patterns of antibiotic utilization on a palliative care unit[J]. J Pain Symptom Manage, 1998, 16(6): 374−381.
[7] Lam PT, Chan KS, Tse CY,. Retrospective analysis of antibiotic use and survival in advanced cancer patients with infections[J]. J Pain Symptom Manage, 2005, 30(6): 536−543.
[8] Yao GH, Peng YN, Tan H. Clinical study of advanced lung cancer patients complicated with lung infection[J]. J Clin Pulm Med, 2013, 18(5): 798−800. [要国华, 彭玉娜, 谭 获. 晚期肺癌合并肺部感染的临床研究[J]. 临床肺科杂志, 2013, 18(5): 798−800.]
[9] Huang Z. Related risk factors for pulmonary infections in cerebral vascular disease patients[J]. Chin J Nosocomiol, 2013, 23(5): 1030−1032. [黄 贞. 脑血管疾病患者合并肺部感染的相关危险因素调查[J]. 中华医院感染学杂志, 2013, 23(5): 1030−1032.]
[10] Chen J, Zhang Y, Sun JH,. Incidence of lung infection in patients with lung cancer and related factors[J]. Chin J Microecol, 2001, 13(2): 120−121. [陈 骏, 张 阳, 孙婧华, 等.肺癌患者肺内感染调查及相关性研究[J]. 中国微生态学杂志, 2001, 13(2): 120−121.]
[11] Wang HM, Liao GQ, Liu PH,. Clinical analysis of low respiratory tract infection in patients with advanced lung cancer[J]. Chin Clin Oncol, 2009, 14(7): 638−640. [王红梅, 廖国清, 刘鹏辉, 等. 晚期肺癌伴下呼吸道感染的临床分析[J]. 临床肿瘤学杂志, 2009, 14(7): 638−640.]
[12] Williams MD, Braun LA, Cooper LM,. Hospitalized cancer patients with severe sepsis: analysis of incidence, mortality, and associated costs of care[J]. Crit Care, 2004, 8(5): R291−R298.
[13] Mercadante S, Fulfaro F, Casuccio A. The use of corticosteroids in home palliative care[J]. Support Care Cancer, 2001, 9(5): 386−389.
[14] Reinbolt RE, Shenk AM, White PH,. Symptomatic treatment of infections in patients with advanced cancer receiving hospice care[J]. J Pain Symptom Manage, 2005, 30(2): 175−182.
[15] Chen LK, Chou YC, Hsu PS,. Antibiotic prescription for fever episodes in hospice patients[J]. Support Care Cancer, 2002, 10(7): 538−541.
[16] Oneschuk D, Fainsinger R, Demoissac D. Antibiotic use in the last week of life in three different palliative care settings[J]. J Palliat Care, 2002, 18(1): 25−28.
[17] Vitetta L, Kenner D, Sali A. Bacterial infections in terminally ill hospice patients[J]. J Pain Symptom Manage, 2000, 20(5): 326−334.
[18] White PH, Kuhlenschmidt HL, Vancura BG,. Antimicrobial use in patients with advanced cancer receiving hospice care[J]. J Pain Symptom Manage, 2003, 25(5): 438−443.
[19] Clayton J, Fardell B, Hutton-Potts J,. Parenteral antibiotics in a palliative care unit: prospective analysis of current practice[J]. Palliat Med, 2003, 17(1): 44−48.
(编辑: 周宇红)
Risk factors of pulmonary infection in elderly patients with terminal stage cancer
YANG Bo*, JIANG Hong-Ning, YU Min, ZHANG Hui-Rong, LONG Lin-Zi
(Department of Hospice Care, Beijing Geriatric Hospital, Beijing 100095, China)
To identify the risk factors of pulmonary infection in the elderly patients with terminal-stage cancer in hospice.Clinical data of 143 elderly patients with terminal-stage cancer hospitalized in our department from October 2012 to November 2013 were collected and retrospectively analyzed. A multivariate logistic regression analysis was carried out in the patients with pulmonary infection (=87) and those without (=56) for the risk factors of pulmonary infection.Variables significantly associated with increased risk of pulmonary infection included lung cancer [odds ratio (OR)=4.137; 95% confidence interval (CI) 1.967 to 14.479), disturbance of consciousness (OR=3.728; 95% CI 1.313 to 8.315), hypoalbuminemia (OR=2.960; 95% CI 1.300 to 6.739), hospital stay (OR=2.611; 95% CI 1.056 to 6.451), performance status (OR=2.187; 95% CI 1.345 to 4.071), diabetes mellitus (OR=1.937; 95% CI 1.159 to 3.238), and chronic obstructive pulmonary disease (COPD; OR=1.823; 95% CI 1.056 to 3.891) in this elderly cohort with terminal stage cancer (all<0.05).Pulmonary infection is common in the elderly patients with terminal stage cancer. Lung cancer, disturbance of consciousness, hypoalbuminemia, prolonged hospitalization, bedridden, and chronic comorbidity (diabetes mellitus and COPD) are risk factors for occurrence of pulmonary infection.
elderly; malignant neoplasms; pulmonary infection; risk factors; hospice care
R592; R48
A
10.3724/SP.J.1264.2014.00085
2014−02−19;
2014−03−05
杨 波, E-mail: yohayohayoha@163.com