氨基末端脑利钠肽前体水平对非HIV免疫损害患者肺炎的预后价值
2014-04-21骆海伦李昱霖梁志欣陈良安
骆海伦,李昱霖,梁志欣,陈良安
解放军总医院 呼吸科,北京 100853
氨基末端脑利钠肽前体水平对非HIV免疫损害患者肺炎的预后价值
骆海伦,李昱霖,梁志欣,陈良安
解放军总医院 呼吸科,北京 100853
目的评价氨基末端脑利钠肽前体(N-terminal pro-brain natriuretic peptide,NT-proBNP)水平对非HIV免疫损害患者肺炎预后的预测作用。方法回顾性研究本院呼吸重症监护病房(respiratory intensive care unit,RICU)2011年1月- 2013年5月收治的非HIV免疫损害患者肺炎的临床资料。收集入RICU 24 h内的NT-proBNP测定值。根据ICU生存情况,分为死亡组和存活组,比较两组间NT-proBNP、APACHEⅡ评分的差异。结果本研究入选患者44例,死亡18例,存活26例。死亡组的NT-proBNP水平(中位数3 066.5 pg/ml)显著高于存活组(中位数372.0 pg/ml)。NT-proBNP和APACHEⅡ评分预测ICU病死率的受试者工作曲线下面积分别为0.707(95%置信区间[0.552,0.862])和0.841(95%置信区间[0.712,0.961])。结论氨基末端脑利钠肽前体水平升高提示预后差,其对非HIV免疫损害患者肺炎的预后价值仍需进一步研究。
免疫损害宿主肺炎;氨基末端脑利钠肽前体;预后
近年来,随着器官移植的开展、肿瘤化疗患者生存时间的延长、糖皮质激素及免疫抑制剂的应用,非人类免疫缺陷病毒(human immunodeficiency virus,HIV)感染导致免疫损害宿主(immunocompromised host,ICH)的数量较前增加。肺是免疫损害宿主最常见的感染靶器官,且病死率较高[1-3]。及时对患者病情严重程度、预后情况作出评估有一定实际意义。脑利钠肽(brain natriuretic peptide,BNP)和氨基末端脑利钠肽前体(N-terminal probrain na-triuretic peptide,NT-proBNP)在心脏疾病的研究方面较成熟[4]。其于脓毒症[5-6]、社区获得性肺炎[7-8]的预后研究已有报道。本研究旨在探讨其对非HIV免疫损害宿主肺炎的预后价值。
资料和方法
1 研究对象及分组 2011年1月- 2013年5月在解放军总医院呼吸重症监护病房住院,有免疫损害病史,有肺部感染的临床表现,胸部影像学显示新发或进展的肺部浸润影,临床诊断为肺炎的患者。排除标准:1)原有肺部基础疾病,且新出现的肺部阴影不能排除为基础病进展所致者;2)慢性充血性心力衰竭患者,慢性肾衰患者(有慢性肾功能受损病史并且最近的肌酐>2.0 mg/dl);3)入呼吸重症监护病房(respiratory intensive care unit,RICU)时存在急性心肌梗死、急性心衰、急性肾衰;4)入RICU当天未检测NT-proBNP者;5)结核病患者、HIV感染者。根据住RICU期间的生存情况,分为死亡组和存活组,病死统计包括住院病死者和抢救无效自动出院者。
2 免疫损害宿主的定义 本研究中的免疫损害宿主为以下患者:1)实体器官或造血干细胞移植术后服用糖皮质激素或免疫抑制剂的患者;2)长期服用糖皮质激素和免疫抑制剂的其他患者,单独应用糖皮质激素者达到≥0.3 mg/(kg·d)的泼尼松龙当量,且至少应用1个月;3)急性白血病患者以及接受积极的细胞毒化疗的肿瘤患者。
3 观察指标 收集年龄、性别、基础疾病等一般资料,入RICU后24 h内NT-proBNP的检测值及各项化验指标(血常规、血气分析、肝功能、肾功能、血电解质等)的最差值。计算入RICU当天的APACHEⅡ评分[9]。
4 统计学方法 采用SPSS13.0软件进行统计分析。正态连续性数据用±s表示,非正态连续性数据用中位数和四分位数间距表示。两组间的比较采用t检验、Mann-Whitney U检验或χ2检验。用受试者工作特征曲线(ROC曲线)下面积评价NT-proBNP水平、APACHEⅡ评分预测病死的价值。以P<0.05为差异有统计学意义。
结 果
1 入选病例基本特征 共收集病例44例,男性23例,女性21例,发病年龄为16 ~ 86岁,平均年龄为49.3岁。肾移植术后7例;血液系统肿瘤9例,其中3例为造血干细胞移植术后;实体肿瘤3例;结缔组织病13例;肾病8例;其他原因服用糖皮质激素、免疫抑制剂4例。44例中既往有冠心病病史5例。
2 死亡组与存活组NT-proBNP及相关因素比较本组患者死亡18例,存活26例。死亡组的NT-proBNP水平(中位数3 066.5 pg/ml)显著高于存活组(中位数372.0 pg/ml)。死亡组的APACHEⅡ评分为18.3±4.8,存活组为12.1±4.1,差异有统计学意义(P=0.000)。死亡组与存活组的年龄、住院时间差异有统计学意义(P值分别为0.040、0.020)。两组间男女患病比例、血肌酐水平差异无统计学意义(P值分别为0.717、0.067)。见表1。
3 NT-proBNP受试者工作曲线(receiver operating characteristic curve,ROC) 分析NT-proBNP、APACHEⅡ评分的ROC曲线下面积分别为0.707(95%置信区间[0.552,0.862])、0.837(95%置信区间[0.712,0.961]),见图1。以NT-proBNP>1 894.0 pg/ml作为预测死亡的界点,灵敏度为61.1%,特异度为73.1%。以APACHEⅡ评分>15作为预测死亡的界点,灵敏度为88.9%,特异度为69.2%。
表1 死亡组与存活组的特征比较Table 1 Clinical parameters of two groups (±s, M)
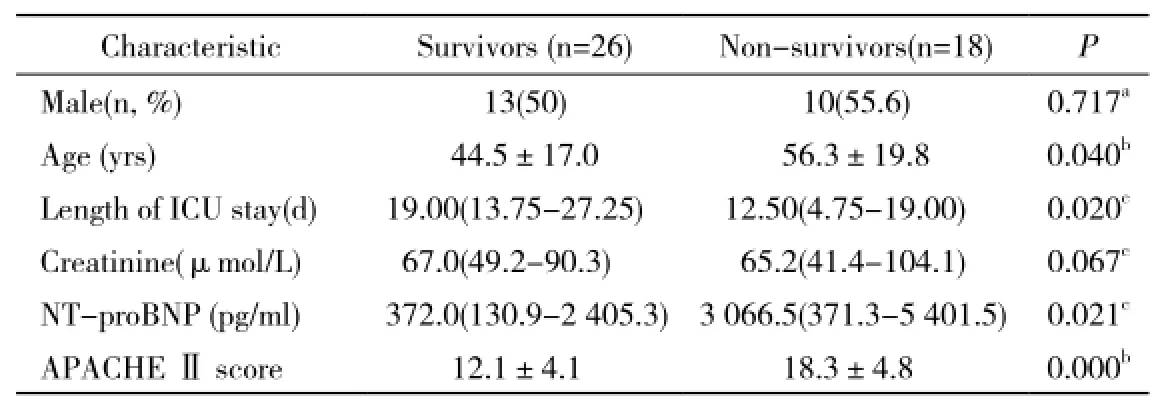
表1 死亡组与存活组的特征比较Table 1 Clinical parameters of two groups (±s, M)
a: Chi Square test; b: Student t test; c: Mann-Whitney U tests; NT-proBNP: N-terminal pro-brain natriuretic peptide; APACHEⅡ: acute physiology and chronic health evaluationⅡ

图 1 NT-proBNP和 APACHEⅡ评分的受试者工作曲线分析Fig. 1 ROC curves for NT-proBNP and APACHEⅡ scores
讨 论
NT-proBNP在临床实验室检测非常方便,较BNP稳定,血清与肝素抗凝血浆检测结果可互换,不同检测方法所得结果的一致性好[10]。关于NT-proBNP与感染的关系的研究以脓毒症居多,NT-proBNP水平升高与脂多糖、促炎细胞因子刺激、液体复苏等相关[5,11]。有Meta分析显示NT-proBNP可以作为脓毒症患者的预后指标[11]。
脓毒症患者是一个异质性非常大群体,就感染部位而言主要为肺和腹部。对于肺炎仍有必要进一步研究NT-proBNP的应用价值。有研究显示NT-proBNP预测社区获得性肺炎的病死率上是有效的[7-8]。对于入住ICU的肺炎患者有研究显示NT-proBNP预测病死率与APACHEⅡ相当[12]。本研究排除心衰、肾衰患者,死亡组的NT-proBNP水平显著高于存活组,说明肺部感染可引起NT-proBNP升高,其升高提示预后差。但本研究NT-proBNP的ROC曲线下面积为0.707(95%置信区间[0.552,0.862]),较APACHEⅡ评分0.837(95%置信区间[0.712,0.961])差,与上述研究结论不同。分析此差异原因为研究人群不同,免疫损害宿主肺炎有免疫受损类型、基础疾病等特殊性,对于免疫损害宿主肺炎,有作者认为应单独归为类[13-14]。Carrabba等[15]在评价肺炎严重指数(pneumonia severity index score,PSI)、CURB-65、重症社区获得性肺炎评分(severe community acquired pneumonia score,SCAP)预测医疗保健相关性肺炎30 d病死率时,发现对于免疫损害组以上评分均较差,并建议为这类患者设计预后模型。另外,免疫损害宿主易并发机会性感染,病原学诊断延迟、不恰当的经验性治疗均与不良预后相关[1,16]。可能是因为免疫损害宿主肺炎的这些特殊性,使得NT-proBNP水平的预后价值降低。
本研究排除了慢性肾衰、急性肾衰患者,并且未发现死亡组与存活组血肌酐水平有统计学差异,在一定程度上排除了肾功能对NT-proBNP的影响,但未对急性肾损伤患者进行分析,有研究显示NT-proBNP与急性肾损伤相关[17]。本研究排除了慢性心衰、急性心衰、急性心肌梗死患者,纳入既往冠心病病史者5例(由于样本量小未作统计学分析),尚不能排除心功能不全的影响。因此需要进一步研究,并对不同心肾功能患者采取亚组分析。
综上所述,NT-proBNP水平在死亡组显著高于存活组,其水平升高提示预后差。但鉴于非HIV免疫损害宿主肺炎的特殊性,NT-proBNP的预后价值仍需进一步研究。
1 Rañó A, Agustí C, Benito N, et al. Prognostic factors of non-HIV immunocompromised patients with pulmonary infiltrates[J]. Chest,2002, 122(1): 253-261.
2 Shorr AF, Susla GM, O’Grady NP. Pulmonary infiltrates in the non-HIV-infected immunocompromised patient: etiologies, diagnostic strategies, and outcomes[J]. Chest, 2004, 125(1): 260-271.
3 Vento S, Cainelli F, Temesgen Z. Lung infections after cancer chemotherapy[J]. Lancet Oncol, 2008, 9(10):982-992.
4 黄学亮,王玲,郭广宏,等.单纯冠心病患者冠脉病变程度与生化指标相关性分析[J].军医进修学院学报,2013,34(1):20-23.
5 Brueckmann M, Huhle G, Lang S, et al. Prognostic value of plasma N-terminal pro-brain natriuretic peptide in patients with severe sepsis[J]. Circulation, 2005, 112(4): 527-534.
6 Varpula M, Pulkki K, Karlsson S, et al. Predictive value of N-terminal pro-brain natriuretic peptide in severe sepsis and septic shock[J]. Crit Care Med, 2007, 35(5): 1277-1283.
7 Nowak A, Breidthardt T, Christ-Crain M, et al. Direct comparison of three natriuretic peptides for prediction of short- and long-term mortality in patients with community-acquired pneumonia[J]. Chest, 2012, 141(4): 974-982.
8 Chang CL, Mills GD, Karalus NC, et al. Biomarkers of cardiac dysfunction and mortality from community-acquired pneumonia in adults[J]. PLoS One, 2013, 8(5):e62612.
9 Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity of disease classification system[J]. Crit Care Med, 1985, 13(10):818-829.
10 Ordonez-Llanos J, Collinson PO, Christenson RH. Amino-terminal pro-B-type natriuretic peptide: analytic considerations[J]. Am J Cardiol, 2008, 101(3A):9-15.
11 Wang F, Wu Y, Tang L, et al. Brain natriuretic peptide for prediction of mortality in patients with sepsis: a systematic review and metaanalysis[J]. Crit Care, 2012, 16(3):R74.
12 Lin SC, Tsai YJ, Huang CT, et al. Prognostic value of plasma N-terminal pro B-type natriuretic peptide levels in pneumonia patients requiring intensive care unit admission[J]. Respirology,2013, 18(6): 933-941.
13 Ewig S, Welte T, Chastre J, et al. Rethinking the concepts of community-acquired and health-care-associated pneumonia[J]. Lancet Infect Dis, 2010, 10(4): 279-287.
14 Yu VL. Guidelines for hospital-acquired pneumonia and health-careassociated pneumonia: a vulnerability, a pitfall, and a fatal flaw[J]. Lancet Infect Dis, 2011, 11(3): 248-252.
15 Carrabba M, Zarantonello M, Bonara P, et al. Severity assessment of healthcare-associated pneumonia and pneumonia in immunosuppression[J]. Eur Respir J, 2012, 40(5): 1201-1210.
16 Li MC, Lee NY, Lee CC, et al. Pneumocystis jiroveci pneumonia in immunocompromised patients: Delayed diagnosis and poor outcomes in non-HIV-infected individuals[J]. J Microbiol Immunol Infect,2012. [Epub ahead of print]
17 Nowak A, Breidthardt T, Dejung S, et al. Natriuretic peptides for early prediction of acute kidney injury in community-acquired pneumonia[J]. Clin Chim Acta, 2013, 419:67-72.
Role of N-terminal pro-brain natriuretic peptide level in predicting prognosis of pneumonia in non-HIV immunocompromised patients
LUO Hai-lun, LI Yu-lin, LIANG Zhiin, CHEN Liang-an
Department of Respiratory Medicine, Chinese PLA General Hospital, Beijing 100853, China Corresponding author: CHEN Liang-an. Email: chenla301@263.net
ObjectiveTo study the role of N-terminal pro-brain natriuretic peptide (NT-proBNP) level in predicting the prognosis of pneumonia in non-HIV immunocompromised patients. MethodsClinical data about pneumonia in non-HIV immunocompromised patients admitted to respiratory intensive care unit(RICU) in our hospital from January 2011 to May 2013 were retrospectively analyzed. The NT-proBNP level in non-HIV immunocompromised patients was measured within 24 h after admission. The patients were divided into death group and survival group according to their mortality in RICU. The NT-proBNP and APACHEⅡscores were compared between the 2 groups. ResultsOf the 44 patients included in this study, 18 died and 26 survived. The NT-proBNP level was significantly higher in death group than in survival group (3 066.5 pg/ml vs 372.0 pg/ml). The area under the ROC curves for the mortality in RICU as predicted with the NT-proBNP and APACHEⅡscores was 0.707 (95% CI: 0.552, 0.862) and 0.841(95% CI: 0.712, 0.961),respectively. ConclusionElevated NT-proBNP level indicate a poor prognosis of pneumonia in non-HIV immunocompromised patients. Its value in predicting the prognosis of pneumonia in non-HIV immunocompromised patients needs to be further studied.
immunocompromised host pneumonia; N-terminal pro-brain natriuretic peptide; prognosis
R 563.1
A
2095-5227(2014)02-0116-03
10.3969/j.issn.2095-5227.2014.02.005
2013-09-16 16:51
http://www.cnki.net/kcms/detail/11.3275.R.20130916.1651.002.html
2013-07-16
全军医学科技“十二五”科研项目(BWS11J057)
Supported by the Military Medical Technology "12th Five-Year" Program (BWS11J057)
骆海伦,男,在读硕士。研究方向:脓毒症。Email: lhl 90202803@163.com
陈良安,男,主任医师,教授,博士生导师。Email: ch enla301@263.net