Can venous blood gas analysis be used for predicting seizure recurrence in emergency department?
2014-03-20
Department of Emergency Medicine, Izmir Tepecik Research and Educational Hospital, Izmir, Turkey
Corresponding Author:Turgay Yılmaz Kılıc, Email: turgayyilmaz.kilic@gmail.com
Can venous blood gas analysis be used for predicting seizure recurrence in emergency department?
Turgay Yılmaz Kılıc, Murat Yesilaras, Ozge Duman Atilla, Mustafa Sever, Ersin Aksay
Department of Emergency Medicine, Izmir Tepecik Research and Educational Hospital, Izmir, Turkey
Corresponding Author:Turgay Yılmaz Kılıc, Email: turgayyilmaz.kilic@gmail.com
BACKGROUND:Epileptic seizures account for 1%–2% of all admissions of patients to the emergency department (ED). The present study aimed to determine whether venous blood pH, bicarbonate, base excess, and lactate levels taken within 1 hour of the last seizure episode help to determine seizure recurrence in emergency departments.
METHODS:A cross-sectional study was conducted in the emergency department (ED) between January and July, 2012. Patients who were admitted to the emergency department consecutively were included in the study if they were 14 years or older and within 1 hour after last seizure. Demographics, seizure type, use of antiepileptic drugs, observation period at the emergency department, seizure recurrence, pH, bicarbonate, base excess, and lactate levels from venous blood gas analysis were determined.
RESULTS:A total of 94 patients aged 14 years or older were included in the study. Of these patients, 10.6% (n=10) experienced recurrent seizures in the observation period at the emergency department. To predict recurrent seizures in ED, threshold venous blood gas values were determined as follows: pH<7.245 [sensitivity 80% (95%CI: 44–96), negative predictive value 96.9% (95%CI: 88.3–99.4)], bicarbonate<17.1 mmol/L [sensitivity 80% (95%CI: 44–96), negative predictive value 97% (95%CI: 89–99.5)], base excess<–11.1 mEq/L [sensitivity 80% (95%CI: 44–96), negative predictive value 97% (95%CI: 89–99)], and lactate>7.65 mmol/L [sensitivity 80% (95%CI: 44–96), negative predictive value 96.6% (95%CI: 87–99)].
CONCLUSION:If venous blood gas analysis is made on pH, base excess, lactate and bicarbonate immediately one hour after the last epileptic seizure episode, it is possible to predict whether the patient will have seizure recurrence.
Seizure recurrence; Venous blood gas; Emergency department
INTRODUCTION
Epileptic seizures account for 1%–2% of all admissions of patients to the emergency department (ED).[1–3]Of the patients, 16.3% were determined to have a recurrent seizure in the ED within 6 hours.[4]Some of the patients with recurrent seizures were hospitalized. Routine laboratory tests revealed that the patients admitted to the ED after a seizure mostly had normal results, and the effect of these tests in patient management was limited.[5–7]All the patients admitted to the ED with seizures were recommended a 4–6 hour observation for seizure recurrence.
Lactic acidosis, metabolic acidosis and respiratory acidosis often develop in patients who have generalized seizures; but these abnormalities typically resolve spontaneously.[8–10]There are no known laboratory tests that accurately predict the probability of the patient having recurrent seizures in the observation period of ED.
This study was undertaken to determine whether venous blood pH, bicarbonate (HCO3), base excess (BE), and lactate levels were taken within 1 hour of the last seizure episode could help to determine seizure recurrence in ED.
METHODS
This cross-sectional study was conducted between January and July, 2012 in the ED of a tertiary referral hospital with an annual admission of approximately 200 000 adult patients. The study was approved by the ethics committee prior to the commencement of the study. Informed written consent was obtained from the patients or their relatives before participating in the study. Epileptic seizure of the patient was diagnosed with the information obtained from the person who witnessed (family members, friends, ambulance officers) muscle spasm and the disturbance of consciousness.
The patients who were consecutively admitted to the ED were included in the study if they were 14 years or older and within 1 hour after the last seizure.
The patients who refused to provide consent form for the study or had seizures secondary to stroke, uremia, electrolyte imbalances, alcohol, trauma, intracranial mass, central nervous system infection, and toxins were excluded from the study. Moreover, the patients who knew nothing about the time of their last seizure episode were excluded. The time of the last seizure was determined by close relatives, friends and ambulance of fi cers.
Venous blood samples were analyzed within the first 5 minutes of ED presentation using the GEM Premier 3000-GEM OPL Co-Oximeter (Instrumentation Laboratory®, USA) for all study participants. The device was calibrated by the manufacturer. Demographics, seizure type, antiepileptic drug use, observation period of ED, seizure recurrence, and pH, HCO3, BE, and lactate levels from venous blood gas analysis were determined.
All statistical analyses were performed with SPSS version 17 (SPSS Inc., Chicago, IL). Qualitative data were expressed as frequency and percentage. Continuous data were expressed as median and interquartile range (IQR) and minimum (min) and maximum (max) values. The Mann-Whitney U test was used for analysis of continuous variables. Receiver operating characteristic (ROC) curves were used for determination of blood gases threshold values and the highest value of sensitivity was selected. All data were analyzed on 95% confidence interval (CI). P<0.05 was considered statistically significant. Statistical power of the study was 85.34% (95% CI) (with Epi Info statistical software v. 3.01).
RESULTS
Altogether 137 patients aged 14 years and older presented to the ED within 1 hour after seizure. Fortythree patients were excluded from the study because they had secondary epilepsy (intracranial mass in 9 patients, intracranial hemorrhage in 8, ischemic stroke in 6, hyponatremia in 1, central nervous system infection in 2, alcohol abuse in 1 and uncertain diagnosis of epilepsy in 16). The remaining 94 patients were included in the study. Fifty-nine of the patients were male (62.8%) and their median age was 32 years (IQR 24 to 50 years; min: 14 years, max: 86 years). Generalized tonic-clonic seizures were diagnosed in 95.5% (n=90) of the patients, and 69.1% of these patients were on antiepileptic drugs.
The median venous blood pH taken at ED presentation was 7.32 (IQR: 7.21 to 7.37; min: 6.91, max: 7.47). The median BE was –3.9 (IQR: –11.7 to 0.78; min: –24.1, max: 6.1), and the median HCO3level was 21.6 (IQR: 16.4 to 26.0; min: 5.5, max: 30.5). Lastly, the median lactate level was 4.3 (IQR: 1.8 to 9.5; min: 0.7, max: 15). According to gender of the patients, median pH, HCO3, BE and lactate values are shown in Table 1.
Of the patients, 10.6% (n=10) experienced recurrent seizures in the ED observation period. There was no statistically significant difference in the incidence of recurrent seizure of male and female patients (respectively 11.9%, 8.6%; P>0.05). Baseline demographic characteristics of these patients are shown in Table 2. According to recurrent seizures of the patients, median pH, HCO3, BE and lactate values are shown in Table 3.
Blood gas values obtained from the ROC curves of the patients with and without seizure recurrence in a follow-up at ED are shown in Figure 1. The sensitivity, speci fi city, positive predictive value (PPV) and negative predictive value (NPV) were calculated from threshold values obtained from the ROC curve analyses of venous blood gas values. These values were obtained from patients with recurrent seizures in the ED observationperiod (Table 4).

Table 1. Median values of blood gas analysis and gender
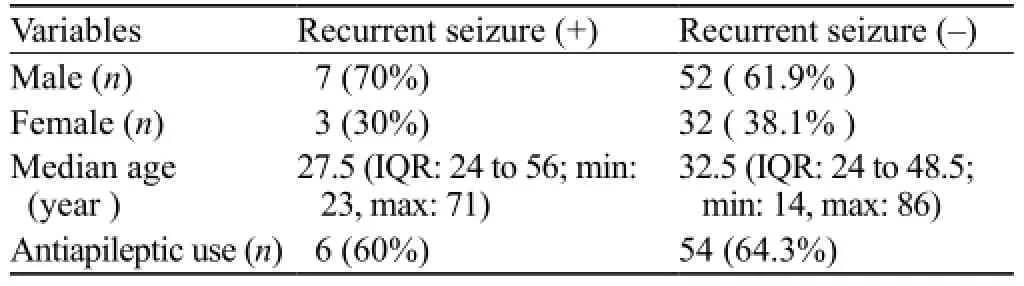
Table 2. Baseline characteristics of the patients with and without seizure recurrence

Table 3. Median values of blood gas analysis for patients with and without seizure recurrence

Table 4. Sensitivity, speci fi city, NPV and PPV for threshold venous blood gas values obtained from patients with recurrent seizures
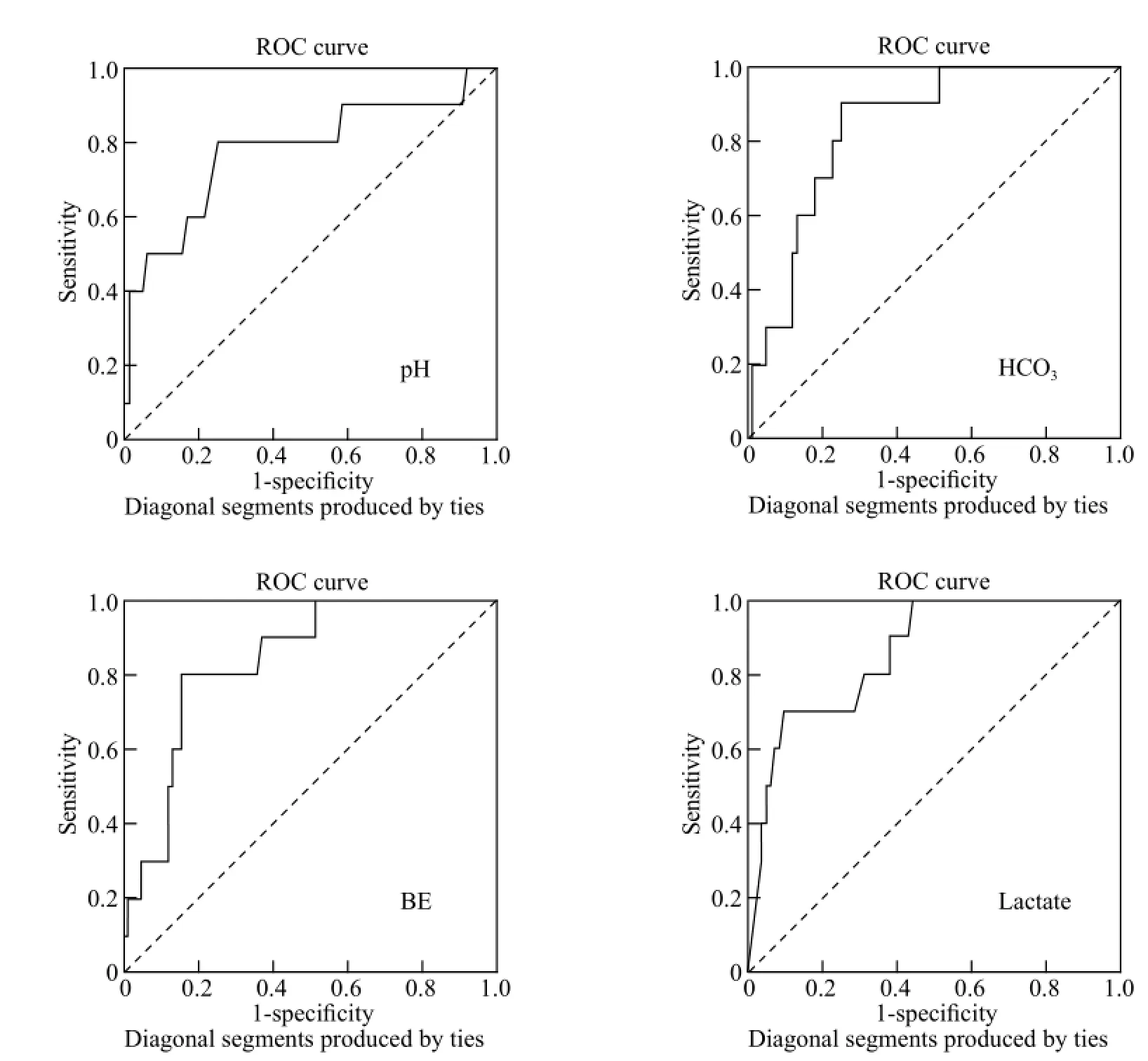
Figure 1. The blood gas values obtained from the ROC curves of the patients with and without seizure recurrence in a ED follow-up.
The median ED observation period was 6 hours (IQR: 6 to 6 hours; min: 2 hours, max: 16 hours). Out of all the patients, 10.6% (n=10) were admitted to the neurointensive care unit. In 10 patients hospitalized, 5 were male (P>0.05) and 7 had recurrent seizures (P< 0.001).
DISCUSSION
This study aimed to evaluate whether blood gas analysis can predict early seizure recurrence in patients with epilepsy. We found that low pH, HCO3, and BE levels in addition to high lactate levels in venous blood drawn within the first hour after the last seizure may predict recurrence in ED.
If a patient experiencing epileptic seizures presents to the ED with venous blood pH, BE and bicarbonate values below 7.245, –11.1 mEq/L, and 17.1 mmol/L, respectively, and a lactate level above 7.65 mmol/L, the patient should be closely monitored. Patients with such venous blood results may be considered at a higher risk for having recurrent seizures and may ultimately be hospitalized.
In the literature, development of severe lactic acidosis and metabolic acidosis in patients with generalized seizures is reported.[9,10]The likely cause of lactic acidosis during a seizure is increased anaerobic metabolism resulting from elevated oxygen utilization during the seizure activity.
Orringer et al[10]determined that lactate levels in venous blood samples drawn immediately after a seizure are signi fi cantly elevated and metabolic acidosis develops. Blood pH values typically return to normal within 1 hour. Metabolic anomalies that occur following an epileptic seizure are self-limited and do not require speci fi c treatment.[11]
Respiratory depression during a seizure may also cause acidosis. Wijdicks et al[8]demonstrated that the most common acid-base imbalance experienced by 32 seizure patients was respiratory acidosis. However, they reported that there was no relationship between the severity of respiratory acidosis and clinical outcomes.
The primary goal of emergency physicians is to control the seizure and to prevent seizure related complications in patients with an epileptic seizure admitted to the ED. After stabilizing the patient, the emergency physicians must determine whether the patient is likely to have recurrent seizures that may necessitate hospitalization. It was reported that alcoholic patients, hyperglycemic patients with plasma glucose levels ≥8.5 mmol/L, or patients who present with Glasgow Coma Scale scores below 15 often have more seizures within the first 24 hours of presenting to the ED.[4]Currently, however, there are no laboratory parameters that can predict whether a patient with epileptic seizures will have a recurrent episode. Therefore, studies, such as ours, are needed in this area.
Higher venous blood lactate levels were seen in males in our study, but pH, BE, and bicarbonate levels were lower in males than in females (Table 1). Although seizure duration was not compared between males and females, it is possible that males at seizures utilize more oxygen as they are more likely to have a greater muscle mass than females. As a result, males demonstrated more likely severe lactic acidosis than females. Although venous blood gas results differed between male and female patients, there were no differences in seizure recurrence according to gender in the period of ED observation. Therefore, we found that differences in venous blood gas values between patients who experienced recurrent seizures or not were not due to gender. Another factor that may contribute to differences in venous blood gas values may be whether the patient experienced additional seizures preceding the seizure episode the patient experienced immediately before presenting to the ED.
The relationship between prolonged and recurrent seizures has not yet been investigated. Prolonged seizures reflect longer durations of epileptic activity, suggesting that the patient has a decreased seizure threshold and that the patient is at risk for seizure recurrence. However, it is unlikely that the exact duration of the seizure episode was noted before the patient presented to the hospital.
The prevalence of hospitalization for patients presenting to the ED with epileptic seizures was found to be 10.6%. The majority of hospitalized patients with seizure are those who experienced recurrent seizures in the ED.
In our study, patients with lower pH, BE, and bicarbonate levels and higher lactate levels than calculated threshold levels seldom experienced recurrent seizures in the 6-hour observation period. Our data suggested that these parameters may help emergency physicians to decide whether these patients require hospitalization or will be discharged from the ED.
The blood gas analyzer could not measure lactate levels greater than 15 mmol/L. As such, blood lactate values above 15 mmol/L were recorded as 15 mmol/L. Because the present study focused on patients with epileptic seizures, the results cannot be generalized to all patients with seizures who present to the ED. Moreover, we did not follow up the patients after they were discharged from the ED, nor we recorded seizure durations while the patients were in the ED.
Abnormal blood gas results may be related to a more prolonged initial seizure or occurrence of recurrent seizures before arrival. This group of patients will have a higher risk of seizure recurrence in the hospital. Hence venous blood gas analysis within the first hour after the last epileptic seizure episode will help emergency physicians to identify the high-risk patients and make correct decisions for the treatment.
Funding:None.
Ethical approval:The study was approved by the local ethics committee.
Conflicts of interest:The authors have no competing interests relevant to the present study.
Contributors:All authors contributed equally to this work. All authors read and approved the fi nal version of the manuscript.
REFERENCES
1 Pallin DJ, Goldstein JN, Moussally JS, Pelletier AJ, Green AR, Camargo CA. Seizure visits in US emergency departments: epidemiology and potential disparities in care. Int J Emerg Med 2008; 1: 97–105.
2 ACEP Clinical Policies Committee; Clinical Policies Subcommittee on Seizures. Clinical policy: Critical issues in the evaluation and management of adult patients presenting to the emergency department with seizures. Ann Emerg Med 2004; 43: 605–625.
3 Huff JS, Morris DL, Kothari RU, Gibbs MA. Emergency department management of patients with seizures: a multicenter study. Acad Emerg Med 2001; 8: 622–628.
4 Choquet C, Depret-Vassal J, Doumenc B, Sarnel S, Casalino E. Predictors of early seizure recurrence in patients admitted for seizures in the emergency department. EJEM 2008; 15: 261–267.
5 Tiamko S, Sawanyawisuth K, Paowana W, Saengsuwan J, Arunpongpaisal S, Chaiyakum A, et al. Seizure presenting to the emergency department, Srinagarind Hospital. J Med Assoc Thai 2006; 89: 362–367.
6 Eisner RF, Turnbull TL, Howes DS, Gold IW. Efficacy of a "standard" seizure workup in the emergency department. Ann Emerg Med 1986; 15: 33–39.
7 Krumholz A, Wiebe S, Gronseth G, Shinnar S, Levisohn P, Ting T, et al. Quality Standards Subcommittee of the American Academy of Neurology; American Epilepsy Society. PracticeParameter: evaluating an apparentunprovoked first seizure in adults (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology 2007; 69: 1996–2007.
8 Wijdicks EF, Hubmayr RD. Acute acid-base disorders associated with status epilepticus. Mayo Clin Proc 1994; 69: 1044–1046.
9 Brivet F, Bernardin M, Cherin P, Chalas J, Galanaud P, Dormont J. Hyperchloremic acidosis during grand mal seizure lactic acidosis. Intensive Care Med 1994; 20: 27–31.
10 Orringer CE, Eustace JC, Wunsch CD, Gardner LB. Natural history of lactic acidosis after grand-mal seizures. A model for the study of an anion-gap acidosis not associated with hyperkalemia. N Eng J Med 1977; 297: 796–769.
11 Lipka K, Bülow HH. Lactic acidosis following convulsions. Acta Anaesthesiol Scand 2003; 47: 616–618.
Received January 20, 2014
Accepted after revision June 3, 2014
World J Emerg Med 2014;5(3):187–191
10.5847/ wjem.j.issn.1920–8642.2014.03.005
杂志排行

World journal of emergency medicine的其它文章
- Domestic versus imported drug-eluting stents for the treatment of patients with acute coronary syndrome
- Comparison of plasma microRNA-1 and cardiac troponin T in early diagnosis of patients with acute myocardial infarction
- International normalized ratio as a predictor of mortality in trauma patients in India
- Knowledge and skills of neonatal resuscitation of health professionals at a university teaching hospital of Northwest Ethiopia
- Relationship between different surgical methods, hemorrhage position, hemorrhage volume, surgical timing, and treatment outcome of hypertensiveintracerebral hemorrhage
- Risk assessment of ischemic stroke associated pneumonia