Prehospital difficult airway management: old things still work
2014-03-17RuggeroCorsoSalvatoreZamponeMarcelloBaccanelliMassimilianoSorbelloGiorgioGambale
Ruggero M. Corso, Salvatore Zampone, Marcello Baccanelli, Massimiliano Sorbello, Giorgio Gambale
1Department of Emergency, Anaesthesia and Intensive Care Section "G.B. Morgagni-Pierantoni" Hospital, Forlì, Italy
2Department of Surgery, Transplantation and Advanced Technologies; Vascular Surgery and Organ Transplant Unit, University Hospital of Catania, Catania, Italy
Corresponding Author:Salvatore Zampone, Email: salvatore.zampone@alice.it
Prehospital difficult airway management: old things still work
Ruggero M. Corso1, Salvatore Zampone1, Marcello Baccanelli1, Massimiliano Sorbello2, Giorgio Gambale1
1Department of Emergency, Anaesthesia and Intensive Care Section "G.B. Morgagni-Pierantoni" Hospital, Forlì, Italy
2Department of Surgery, Transplantation and Advanced Technologies; Vascular Surgery and Organ Transplant Unit, University Hospital of Catania, Catania, Italy
Corresponding Author:Salvatore Zampone, Email: salvatore.zampone@alice.it
To the Editor:
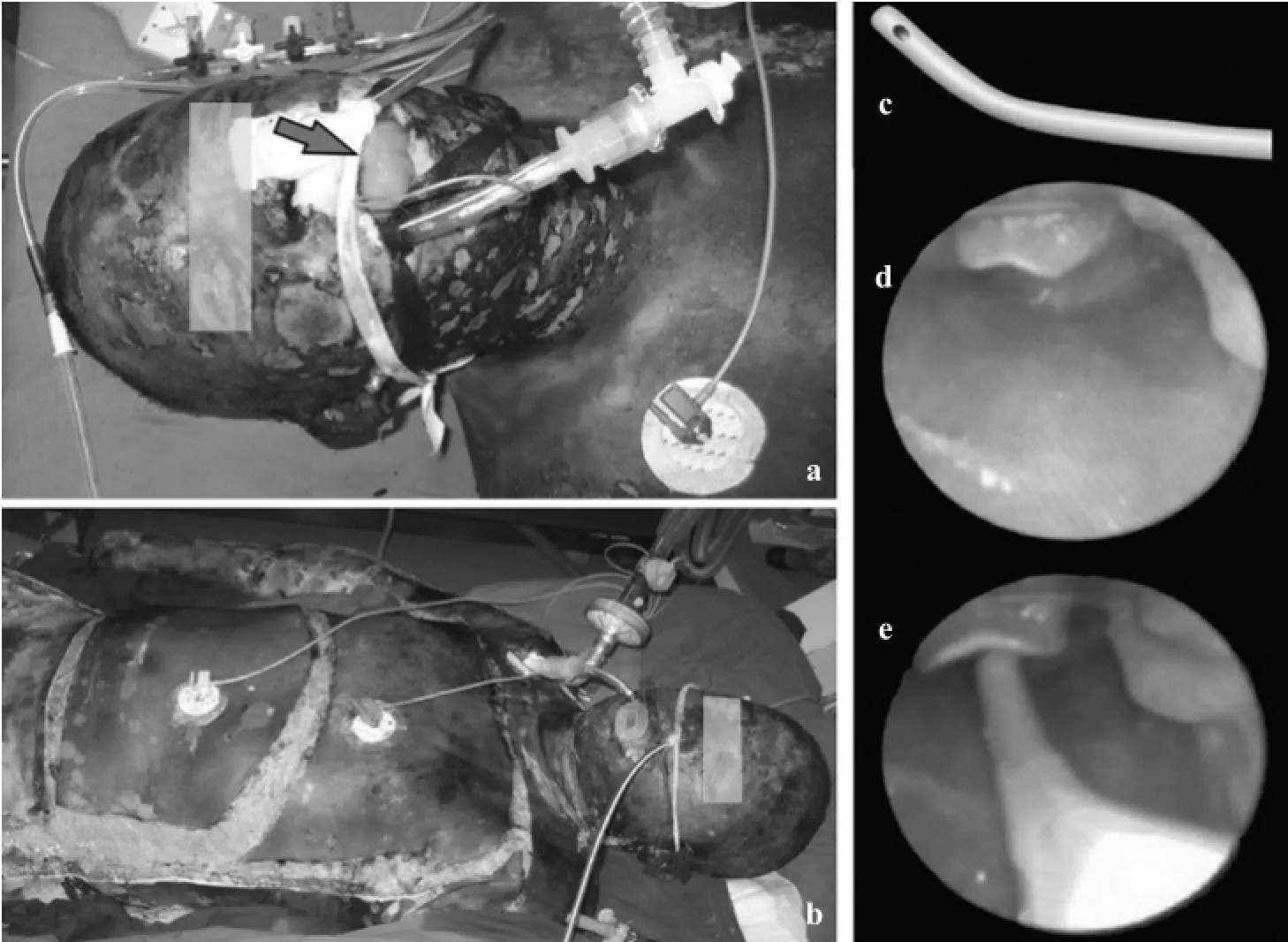
Figure 1. A patient showing extensive burns, with a tracheal tube in situ; note tongue edema (a, b); Frova introducer: particular of the bent tip (c); simulation of CL3 grade view and Frova introducer passing on the midline below the epiglottis (d, e).
Airway management is a crucial skill for emergency physician, who's often called to deal with difficult airways and requests for quick, simple and effective responses, as the many factors responsible for difficulties might be enhanced by emergency setting.[1]We now have many rescue devices as the LMA, I-gel, but they do not provide a definitive airway, and recent studies evaluating the use of the videolaryngoscopes in emergency show conflicting results.[2]In contrast, endotracheal tube introducers or "Gum Elastic Bougies" (GEBs) are simple and inexpensive airway management tools that are used in cases of unanticipated difficulty. The Frova introducer (FI) (Cook®Medical, Bloomington, USA) is a commonly used example and has a high success rate for tracheal intubation in manikins.[3]We usedfiin the prehospital airway management of a 40-year-old man severely burned while working in a weeds field. He sustained full-thickness (third-degree) burns over 98% of his body (Figure 1 a-b). The emergency prehospital rescue team of an anesthesiologist and two nurses found the patient lying on the ground. Initial vital signs were: pulse 130 per minute, respiration 36 per minute, blood pressure (S/D) 153/90 mmHg, andarterial oxygen saturation 80%. The initial Glasgow Coma Scale (GCS) was 10. The extensive burns of the face and the neck resulting in gross edema with inspiratory stridor call for immediate action to secure the airway. After initial bag-mask oxygenation, blow by oxygen (12 L per minute), the crew elected to perform a rapid sequence induction (RSI) with Frova-assisted orotracheal intubation. An intubation laryngeal mask and a surgical airway kit were at hand in case of failure. After a single intravenous bolus of ketamine (2.0 mg/kg) and succinylcholine (1 mg/kg), a direct laryngoscopy was attempted. The laryngoscopic view showed a 3 Cormack-Lehane grade:fiwas then gently pushed on the midline below the visible part of the epiglottis, and the tracheal tube railroaded over it, allowing a successful intubation of the trachea, as confirmed by capnography. Continuous sedation with midazolam and fentanyl was started and the patient was referred to the Burn Centre for definitive care. Airway management in the emergency prehospital setting is often more difficult than that in the operating room. Breckwoldt et al[1]in a physician-based emergency medical system (EMS) found an incidence of difficult tracheal intubation of 13%, and an incidence of unexpected difficulty of 5%. Recently, the use of GEB in a prehospital difficult intubation algorithm has been validated,[4]however in that study the type of GEB is not specified mistakenly assuming that all GEBs are equally effective. To our knowledge, this is the first description of the use offiin the prehospital setting. Its shape, stiffness and tip's curvature were designed to facilitate the transformation of gentle force applied to the proximal end into an anterior and upward directed movement at the distal end, resulting in a smooth shift towards a partly or completely covered laryngeal inlet (Figure 1). Also, the presence of a hollow lumen may prove useful to confirm proper tracheal placement. There may be however potential for tissue trauma, suggested by both manikin studies and case reports in the literature. Proper technique of use is critical to minimize the risk of airway trauma.[5]We think that, despite high-tech (and more expensive) gadgets growing popularity and diffusion, the “old” Frova intubating introducer, being handsized and easy to carry, simple to use and cheap airway device, might be a useful tool for prehospital airway management.
Funding:None.
Ethical approval:Not needed.
Conflicts of interest:The authors have no commercial associations or sources of support that might pose a conflict of interest.
Contributors:All authors have made substantive contributions to the study, and all authors endorse the data and conclusions.
REFERENCES
1 Breckwoldt J, Klemstein S, Brunne, B. Schnitzer L, Mochmann HC, Arntz HR. Difficult prehospital endotracheal intubation -predisposing factors in a physician based EMS. Resuscitation 2011; 82: 1519–1524.
2 Trimmel H, Kreutziger J, Fertsak G., Fitzka R, Dittrich M, Voelckel WG. Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: a randomized control trial. Crit Care Med 2011; 39: 489–493.
3 Janakiraman C, Hodzovic I, Reddy S, Desai N, Wilkes AR, Latto IP: Evaluation of tracheal tube introducers in simulated difficult intubation. Anaesthesia 2009; 64: 309–314.
4 Combes X, Jabre P, Margenet A, Merle JC, Leroux B, Dru M, et al. Unanticipated difficult airway management in the prehospital emergency setting: prospective validation of an algorithm. Anesthesiology 2011; 114: 105–110.
5 Sorbello M, Frova G. Frova introducer: neither a stylet nor simpy an introducer. Anaesthesia 2008; 63: 1010–1011.
Received September 12, 2013
Accepted after revision January 19, 2014
杂志排行

World journal of emergency medicine的其它文章
- Wilderness medicine
- Lean techniques for the improvement of patients'flow in emergency department
- The knowledge level offinal year undergraduate health science students and medical interns about cardiopulmonary resuscitation at a university teaching hospital of Northwest Ethiopia
- Strategic planning and designing of a hospital disaster manual in a tertiary care, teaching, research and referral institute in India
- Effects of early rehabilitation therapy on patients with mechanical ventilation
- Bispectral index in predicting the prognosis of patients with coma in intensive care unit