Incidence investigation and analysis of hepatic stress injury after trauma
2012-07-25WANGQuanchuZHANGYafeiCHENGZhengxiang
WANG Quanchu,ZHANG Yafei,CHENG Zhengxiang
Department of Infectious Diseases,153th Hospital of PLA,Zhengzhou 450042,China
It has been reported in clinic that hepatic injury is not rarely seen in patients with severe trauma.However,in most cases,it is still a problem to which surgeons have not paid sufficient attention.In this study,we reviewed the incidence and characteristics of hepatic stress injury(HSI)secondary to trauma in 4 677 patients in 153th Hospital of PLA from Jan.2004 to Jul.2005,and furthermore,in combination with medical information,we analyzed the possible pathogenesis of the HSI.
1 Materials and Methods
1.1 Cases resource 4 677 inpatients(3 118 men and 1 559 women,aging from 4 to 68 years)in 153th Hospital of PLA from Jan.2004 to Jul.2005 were enrolled in this study.Causes of injury included head injury(780 cases),bone injury(995 cases),hand injury(1 500 cases),abdominal injury(599 cases),thoracic injury(701 cases)and burn injury(102 cases),among which,4 532 cases were referred for surgical treatment,and the left 145 cases were referred for non-surgical treatment.After treatment,the outcome was considered cured in 4 649 cases,moderate disabled in 18 cases,severe disabled in 2 cases and dead in 8 cases.
1.2 Investigation methods Statistical analysis was done on the liver function test results of all the trauma patients.The inspection items in the liver function test included total protein,albumin,globulin,albumin/globulin ratio,alanine aminotransferase(ALT),aspartate aminotransferase(AST),ALT/AST ratio,total bilirubin,direct bilirubin,indirect bilirubin,lactate dehydrogenase(LDH),gamma glutamyl transferase(GGT),alkaline phosphatase(ALP)andmonoamineoxidase(MAO).Further,we analyzed the etiology and possible pathogenesis in combination with the medical information of the patients occurred liver dysfunction.
1.3 Statistics All statistical analyses were performed using SPSS 11.0 software(Chicago,IL,USA).P <0.05 was considered as statistically significant.
2 Results
The main manifestation of liver dysfunction was the elevated ALT or AST levels(387 cases,8.3%).In the various causes,the incidence of liver dysfunction after hand injury was 16.6%,which was statistically higher than that in other causes.The incidence of burn injury,head injury,bone injury,abdominal injury,and thoracic injury were 6.9%,5.6%,5.0%,3.8%and 2.0%,respectively,which was no difference in statistics(Tab 1).Part of the 387 patients had decreased levels of total protein and albumin(110 cases,28.4%),or increased total bilirubin(19 cases,4.9%).Five patients which occurred obvious jaundice had the history of hepatitis B(anti-HBs or anti-HBc positive),and the left 14 patients with increased total bilirubin all excluded the history of hepatitis B.Majority of the liver dysfunction were found at the next day after trauma(352 cases,91.0%),and minority was found at the second or third week after admission(35 cases,9.0%).Among the 387 casess,after stopping or reducing the use of drugs inducing hepatic injury and the application of drugs protecting liver functions,most(268 cases,69.3%)recovered in the first or second week,and the left(119 cases,30.7%)recovered in the third or fourth week.
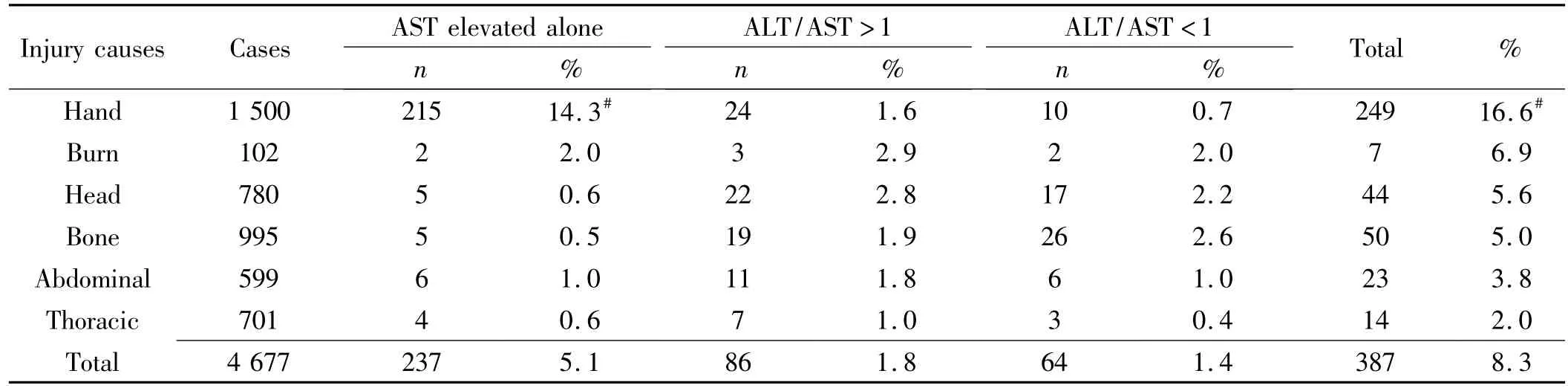
Tab 1 The liver dysfunction in 4 677 patients after severe trauma
3 Discussion
As we all known,various complications can occur following severe trauma.Previous studies revealed that hepatic injury after severe trauma included liver dysfunction,cholestasis,increased hepatic acute-phase proteins,hepatic reticuloendothelial system dysfunction,disturbance of hepatic cytochrome P450 function and hepatohemia,and the clinical manifestations included liver failure,hepatitis,cholestasis and hepatorenal syndrome.E-ven the pathogenesis is still not clear,hepatic stress injury(HSI),as an important part of stress response to trauma,should be paid close attention,just as did stress gastric ulcer.Intestinal endotoxemia might be one of the beginning componentsofHSI. Endotoxins, otherwise termed“lipopolysaccharides(LPS)”,are part of the outer membrane of the cell wall of gram-negative bacteria in intestinal tract.In severe trauma,infection and other stress conditions,because intestinal mucosal barrier is impaired,large amount of endotoxin released in the intestine intrudes into general circulation trough portal vein,inducing damage to the whole body,among which,liver is one of the main affected organs.
3.1 Traumatic head injury and liver dysfunction There is great difference in the reported incidence of liver dysfunction after traumatic head injury,ranging from 2%to 47%[1].In this study,the incidence is 5.6% .And according to our observation,most of the liver dysfunction secondary to head injury occurred in the early stage after trauma and was closely correlated with the severity of injury.All the patients gradually recovered in one month,and none died of liver dysfunction.The mechanisms of liver dysfunction after traumatic head injury are not clear until now.It might relate to the following factors:(1)Cytokines:clinical and experimental researches have revealed that the levels of cytokines such as IL-1,IL-6,IL-8 and TNF in serum and brain increased obviously after traumatic head injury,which induced damage in not only brain but also liver.Therefore,cytokines might be the etiology of liver dysfunction after traumatic head injury.(2)Free radicals:after traumatic head injury,the level of free radicals in serum was elevated,either in liver tissue,and when the level exceeded the capacity of free radical scavenging,liver damage occurred.(3)Arachidonic acid:the plasma arachidonic acid level was increased after traumatic head injury,which induced liver damage through formation of prostaglandins,thromboxane,and leukotriene.(4)Endothelin:the plasma endothelin level was increased significantly after traumatic head injury.Endothelin could promote glycogenolysis and increase the oxygen consumption of liver,thus leading to the increase of cellular Cat level.For that,endothelin could disturb the energy metabolism in liver cells,which ultimately induced the damage of liver cells.Taken together,multiple factors might be involved in the development of liver dysfunction after traumatic head injury.
3.2 Burn injury and liver dysfunction The incidence of acute liver dysfunction after severe burn injury is high according to previous reports,with a mean of 28.56%[2].In this study,various degrees of liver dysfunction occurred in 7 of the 102 patients with severe burn injury(6.9%),indicating that liver is also easily injured after burn injury.Due to damage resulting from hepatic ischemia,infection and toxic substances,the function of hepatic mononuclear phagocyte system was inhibited,which resulted in the decrease of inactivation of endotoxin.Because of the impaired intestinal mucosal barrier,endotoxemia happened at the same time,which further shocked the liver function.In addition,infections,bacteria and toxins after burn injury induced the activation of Kupffer cells,which could produce large amount of inflammatory cytokines,such as TNF-α.TNF-α is the main cytokine involved in the endotoxin-induced acute liver damage.As activators,TNF-α and endotoxin induced non-specific hypersensitivity in liver,which leaded to local microcirculation.Moreover,TNF-α could activate phospholipase,by which,it induced the expression of a series of cytokines,thus aggravating the liver dysfunction.
3.3 Multiple trauma and liver dysfunction Due to the influence of shock,phagocytes activation,inflammatory cytokines releasing,toxin-absorbing,and ischemiareperfusion,which often occurred subsequently following severe multiple trauma,HSI is not rarely.The mild cases showed elevated serum bilirubin and changes in aminotransferase levels.For the severe cases,coagulation factors and albumin were decreased either,and for some,liver failure would ultimately happen.On one hand,the liver dysfunction owned to the direct damage of liver cells and/or the indirect damage induced by cytokines.On the other hand,in the condition of stress,the blood flow in liver was reduced,for which,ischemic and hypoxia occurred in liver tissue,resulting in the damage of liver function[3].Over all,protecting the liver from any possible damage is important for the treatment of patients with multiple trauma.It may delay the progression of the condition,and earn more treatment opportunities,for which,we may improve the rate of successful rescue greatly.
3.4 Hand injury and liver dysfunction The mechanisms under liver dysfunction after hand injury are not yet clear.In this study,215 cases were observed an elevated AST level,with ALT level normal(14.3%),which was significantly higher than that in other injuries.We hypothesized that the phenomenon might be associated with the distribution of ALT in skeletal muscle,for the incidence of elevated ALT/AST ratio,which represented the liver dysfunction better,was not different from other injuries.
In conclusion,it is important for surgeons to pay close attention to HIS.When liver dysfunction has appeared,drugs that are harmful to liver should be ceased or reduced,to avoid the aggravation of liver dysfunction,and correspondingly,it may be useful to treat these patients with drugs protecting liver function.Additionally,in clinic,monitoring of liver function should be applied conventionally,by which,liver dysfunction could be discovered and treated in an early stage.Liver ischemic injury maybe another incentive of HSI which need further investigation.
[1] Gao WY.Complications of digestive system.Therapy and rehabilitation of sever burn[M].Beijing:Science Press,2000:196-197.
[2] Hei YR,Hou XB,Tan HM.Experimental study on irritable hepatic injury after chest explosive trauma[J].Chin J Crit Care Med,2003,23(1):10-13.
[3] McVicker BL,Tuma PL,Kharbanda KK,et al.Relationship between oxidative stress and hepatic glutathione levels in ethanol-mediated apoptosis of polarized hepatic cells[J].World J Gastroenterol,2009,15(21):2609-2616.