Injury rate,mechanism,and risk factors of hamstring strain injuries in sports:A review of the literature
2012-07-06HuiLiuWillimGrrettCludeMoormnBingYu
Hui Liu ,Willim E.Grrett,Clude T.Moormn ,Bing Yu *
a Sports Biomechanics Laboratory,College of Human Movement Science,Beijing Sport University,Beijing 100084,China
b Sports Medicine Center,Duke University,Durham,NC 27710,USA
c Center for Human Movement Science,The University of North Carolina at Chapel Hill,Chapel Hill,NC 27599,USA
Injury rate,mechanism,and risk factors of hamstring strain injuries in sports:A review of the literature
Hui Liua,William E.Garrettb,Claude T.Moormanb,Bing Yuc,*
aSports Biomechanics Laboratory,College of Human Movement Science,Beijing Sport University,Beijing 100084,China
bSports Medicine Center,Duke University,Durham,NC 27710,USA
cCenter for Human Movement Science,The University of North Carolina at Chapel Hill,Chapel Hill,NC 27599,USA
Hamstring strains are one of mostcommon sports injuries.The purpose of this literature review is to summarize studies on hamstring strain injury rate,mechanism,and risk factors in the last severaldecades with a focus on the prevention and rehabilitation of this injury.Hamstring injury commonly occurs in sporting events in which high speed sprinting and kicking are frequently performed,such as Australian football, English rugby,American football,and soccer.Basic science studies have demonstrated thata muscle strain injury occurs due to excessive strain in eccentric contraction instead of force,and thatelongation speed and duration of activation before eccentric contraction affectthe severity of the injury.Hamstring strain injury is likely to occur during the late swing phase and late stance phase of sprint running.Shortened optimum muscle length,lack of muscle flexibility,strength imbalance,insufficient warm-up,fatigue,lower back injury,poor lumbar posture,and increased muscle neuraltension have been identified as modifiable risk factors while muscle compositions,age,race,and previous injuries are non-modifiable risk factors.The theoretical basis of some of these risk factors,however,is lacking,and the results of clinical studies on these risk factors are inconsistent.Future studies are needed to establish the cause-and-effectrelation ships between those proposed risk factors and the injury.
Copyright©2012,Shanghai University of Sport.Production and hosting by Elsevier B.V.All rights reserved.
Hamstring injury;Mechanism;Prevention;Rehabilitation;Sport medicine
1.Introduction
Hamstring strain injury is one of the most common injuries in sports,and causes significant loss of training and competition time and significantly affects the quality of life of injured athletes.This indicates a need to prevent thisinjury.Hamstring muscle injury also has a high re-injury rate, which frustrates the injured athletes as well as the clinicians and increases cost of the treatment.This indicates a need to improve current prevention and treatment strategies for hamstring strains.To prevent hamstring strain injury and improve the treatment for this injury,understanding the injury rate,mechanisms,and risk factors is essential. Significant research efforts have been made to understand hamstring muscle strain injury and re-injury over the last several decades.These research efforts provided further insight into prevention,treatment and clinical practice.The purpose of this literature review is to summarize studies on hamstring strain injury rate,mechanism,and risk factors with a focus on the prevention and rehabilitation of this injury.
2.Injury rate
A hamstring muscle strain injury is defined as posterior thigh pain,where direct contact with the thigh is excluded as a cause of the injury,with hyperintense within the hamstring muscle(s)that can be detected in magnetic resonance imaging (MRI).1Hamstring injuries are often diagnosed based on clinical and/or ultrasound examinations.They commonly occur in the athletes of many popular sport events in which high speed sprinting and kicking are frequently performed, including Australian football,English rugby,soccer,and American football.
Hamstring muscle strain injury is the most common and prevalentinjury in Australian football.Verralletal.2reported that 30%of Australian football players in two clubs had posterior thigh pain over one season.Orchard and Seward3reported a hamstring muscle strain injury rate of six injuries per club per season in Australian football between 1997 and 2000.Hoskins and Pollard4reported the same injury rate between 1987 and 2003.Gabbe et al.5found that 16%of Australian football players sustained hamstring muscle strain injuries during the 2000 season alone with an incidence offour injuries per 1000 player hours.
Hamstring injuries are also very common in English rugby. Brooks et al.6reported an incidence of 0.27 hamstring muscle strain injuries per 1000 player training hours and 5.6 injuries per 1000 player match hours,respectively,between 2002 and 2004.They also reported that,on average,hamstring muscle strain injuries resulted in 17 days oflosttraining/playing time. Their results indicate that the hamstring muscle strain injury was the second most commonly seen injury in English rugby.
Woods etal.7,8found thathamstring strain injury accounted for11%of the totalinjuries in preseason trainings,and 12%of the total injuries in competition seasons in English professional soccer.A total of 13,116 days and 2029 matches were missed because of these injuries with an average of 90 days and 15 matches missed per club per season and 18 days and three matchesmissed perinjury.Arnason etal.9and Dadebo etal.10also reported that hamstring strain injuries represented 11% of all injuries in professional soccer in England,13%in Norway,and 16%in Iceland,respectively.Ekstrand and Gillquist11revealed that hamstring strain injury represented 17%of all injuries and presented in 12%of players in soccer in Europe.The results of these studies demonstrate that hamstring strain injury is among the most common acute injuries in European soccer.
Hamstring muscle strain injury is also common in American football.A review of the medicaldatabase of the National FootballLeague(NFL)between 1987 and 2000 indicated that 10%of allinjuries in American college footballplayers likely to play in the NFLwerehamstring strain injuries.12Feeley etal.13reported that 12%of all injuries in NFL training camps were hamstring strain injuries,making it the second most commonly seen injury.Elliott et al.14reported that the average hamstring strain injury rate of NFL players during a 10-year period was 0.77 per 1000 athlete-exposure and represented 13%of all injuries among NFL players.
Many studies have also reported that hamstring muscle strain injury frequently occurs in many popular individual sports,such as track and field,waterskiing,cross-country skiing,downhill skiing,judo,cricket,and bull riding.15—21Besides sports,dancing is another physical activity that has a high risk for hamstring muscle strain injury.Askling et al.22reported that 34%of dancers have experienced acute hamstring strain injuries and 17%had overuse injuries of hamstring muscles.
3.Recurrence rate
Hamstring strain injury has a very high recurrence rate.In English professionalsoccer,hamstring strain injury reoccurred in between 12%and 48%of the players.8,10,23,24The recurrence rate of hamstring strain injury has been reported to be two times higher than that of other injuries in English professionalsoccer.8In Australian football,34%of the players reinjured theirhamstring muscles within a yearofreturning to play after their initial hamstring strain injuries.3Australian football players had the highest risk(13%)of recurrence of hamstring muscle strain injury during the first week of returning to play.25In addition,the persistence of the recurrence was reported to continue for many weeks after returning to play with a cumulative recurrence risk of 31%over the entire season in comparison to 15%,12%,11%,and 5%of recurrence risks for ankle sprain,thigh contusion,medial collateral ligament strain,and concussion,respectively.25Recurrent hamstring muscle strain injuries are generally more severe and result in significantly more lost time in comparison to the initial injury.25
4.Consequences of the hamstring muscle strain injury
The consequences of a hamstring muscle strain depend on the severity of the injury.There is no standardized classification system for the severity of muscle strain injuries;however, different classification systems share a common categorization.Combining anatomical diagnosis,physical examination, ultrasound,and imaging,the severity of muscle strain injuries is generally categorized as Grade I:mild strain injury with minimum tear of the musculotendinous unit and minor loss of strength,Grade II:moderate strain injury with a partial tear of the musculotendinous unit and a significant loss of strength thatresults in significant functional limitations,and Grade III: severe strain injury with a complete rupture of the musculotendinous unit and is associated with severe functional disability.26,27The precise definitions of different grades may vary among specific classification systems.The averaged time losses for different grades of hamstring muscle strain injuries in European professionalsoccer are 17±10 days for Grade I, 22±11 days for Grade II,and 73±60 days for Grade III.28
The majority(97%)of all hamstring strains in soccer are classified as grade I and grade II.29The complete tear of the hamstring muscle is rare,occurring in roughly 1%of all hamstring injuries,however,the consequences are usually much more severe.8Grade IIIinjuries can resultin an avulsion fracture of the ischium,an avulsion of the ischialapophysis,or a pure avulsion of the hamstring tendons themselves, depending on the patient’s age.30The rare incidence of complete rupturing of the hamstring is often misdiagnosed as a simple“hamstring pull”,resulting in improper treatment thereby leading to the development of chronic pain and potential disability.30
Because the symptomsofa grade Iand grade IImuscle strain injuries may be negligible or entirely absent at rest or in activities of daily living,the patientmay prematurely return to activity.This may lead to repeatedly unsuccessful efforts to return to sports,resulting in re-injuries or a development of chronicity of the injury and symptoms,even longer rehabilitation times,and,in worstcases,the end of an athletic career.31Muckle32pointed out that recurrent hamstring injuries may cause lumbar spine abnormalities,meniscal problems in the knee,adhesion of the lateral popliteal nerve,abnormal quadriceps power,and enthesopathies.Hernesman etal.33reported a case of motor dysfunction of the sciatic nerve from a chronic hamstring strain injury.Petersen et al.34reported 46 new and eight recurrent injuries resulting in a total of 1163 days of absence from football(ranging from 3 to 136 days with a mean of 21.5 days and a median of 16 days per injury)among 374 elite Danish soccer players over a 12-month period.
5.General mechanism of muscle strain injury
Understanding the general mechanism of muscle strain injury is essential for understanding the specific mechanisms ofhamstring muscle strain injury.Tremendous research efforts have been made in the last two decades to understand the general mechanism of muscle strain injury.The results of previous studies demonstrate that muscle strain in eccentric contraction is the primary cause of the muscle strain injury affected by muscle strength and contraction velocity.
Garrett et al.35studied the biomechanics of muscle strain injury using rabbit extensor digitorum longus and tibialis anterior models.They compared the strain,force,and energy absorbed at the time the muscle was stretched to the point of injury in three experimentalgroups:passive stretching group, eccentric contraction group stimulated at 16 Hz,and eccentric contraction group stimulated at 64 Hz.Muscle strain injury was defined as the increase of muscle length from the muscle resting length divided by the muscle resting length.Muscle resting length was defined as the muscle length at which the muscle parallel element starts to generate force as muscle length increases.All injuries occurred at the distal muscletendon junctions with minimum deformation in the tendons. The results of this study showed no significant differences in muscle strain among the three groups when muscle strain injury occurred.The results of this study also showed thatthe force generated by the eccentric contraction groups when muscle strain injuries occurred was significantly greater than thatby the passive stretch group,and thatthe forces generated by the two eccentric contraction groups were notsignificantly different.The results of this study further showed that the eccentric contraction groups absorbed significantly more mechanical energy before injury occurred,and that the eccentric contraction group at the higher activation level absorbed significantly more mechanical energy than the eccentric contraction group atthe lower activation level.These results suggest that muscle strain is the primary cause of the injury regardless of the muscle activation level.These results also suggestthata muscle generates greater force in eccentric contraction than in passive stretch when a muscle strain injury occurs,and that the force a muscle generated in eccentric contraction when a muscle strain injury occurs is not affected by the muscle activation level.These results further suggest thatthe higherthe activation levelofa muscle during eccentric contraction,the more mechanical energy the muscle would absorb before a muscle strain injury occurs.A later study by Lieber and Friden36also demonstrated that lower grade muscle strain injury similar to that of delayed onset muscle soreness was sensitive to the strain not the force.
As a continuation of their previous study,Nikolaou etal.37compared the strain injury sites and muscle strain at failure among rabbit anterior tibialis,extensor digitorum longus, rectus femoris,and gastrocnemius muscles that represent four architectures:fusiform,unipennate,bipennate,and multipennate.The results of this study showed thatmore than 97% of strain injuries in the anterior tibialis,extensor digitorum longus,and rectus femoris occurred at the distal muscletendon junction while only 55%of the injuries in the gastrocnemius occurred in this region.The other45%involved distal as well as proximal muscle-tendon junctions.The elongation speed did not affect where an injury occurred.
Best et al.38studied the effects of elongation speed on the biomechanicalcharacteristics of the muscle strain injury using a rabbit anterior tibialis model.The results of this study showed that muscle material failure occurred at the distal muscle-tendon junction when the elongation speeds were at4 and 40 cm/s,and that failure occurred at the distal muscle belly when the elongation speed was at 100 cm/s.The results of this study also showed that the external loading at failure was sensitive to elongation speed,and that the greater the elongation speed was,the greater the external loading at failure.These results suggest that the muscle strain injury site moves toward proximal from distal muscle-tendon junction while muscle elongation speed is increasing,and that the greater the elongation speed is,the greater the muscle contraction force when injury occurs.This study further showed that the total muscle axial deformation and strain at failure were not elongation speed sensitive.This result was likely due to a low statistical power in the data analysis.The data showed a trend that the total muscle axial deformation and strain at failure decreased as the elongation speed increased,which indicates that muscle strain injury may occur with less muscle strain as elongation speed increases.
Brooks and Faulkner39investigated the effects of muscle elongation speed during eccentric contraction on the severity of muscle strain injury using a mouse extensor digitorumlongus model.The severity of a muscle strain injury was quantified by the deficit in maximum isometric contraction after the injury.Their results showed that the deficit in the maximum isometric contraction force after a muscle strain injury could be predicted from the muscle strain and elongation speed during the eccentric contraction that induced the injury.The role of muscle elongation speed in predicting the deficit in maximum isometric contraction force after a muscle strain injury depended on the muscle strain.The contribution of the muscle elongation speed to the prediction of the severity of strain injury increased as the muscle strain increased when muscle strain was large.These results suggest that the greater the muscle elongation speed in an eccentric contraction is,the more severe the muscle strain injury willbe when the muscle strain is large.
Lovering et al.40studied the effect of muscle activation before eccentric contraction on the severity of muscle strain injury using a rat tibialis anterior model.The degree of injury was also determined by the loss of the maximum isometric contraction force after the injury.The results showed a significant negative correlation between the duration of the muscle activation before eccentric contraction and the amount of loss of the maximum isometric contraction force after the injury,particularly when the duration of muscle activation was less than 50 ms before the eccentric contraction.These results indicate that a suddenly activated eccentric contraction is more likely to cause severe muscle strain injury.
6.Mechanism of hamstring strain injury
The majority of hamstring muscle strain injuries occur in sports that require high speed running such as American football, Australia football,basketball,soccer,rugby,and track and field.41Verrall et al.42reported that 65 out of 69 confirmed hamstring muscle strain injuries during two playing seasons of Australia football occurred during running activities.Gabbe etal.5reported thatover80%oftheconfirmed hamstring musclestrain injuriesin community level Australia football occurred in running or sprinting.Woods etal.8reported thatover 60%of the hamstring injuries occurred during running in English professional soccer. Brooks etal.6reported thatover 68%of hamstring muscle strain injuries in English rugby occurred during running,notincluding turning and scrimmaging which are similarto running.Askling et al.31identified 18 athletes who had first time hamstring muscle strain injuries from majortrack and field clubs in Sweden.All18 athletes were sprinters,and their injuries all occurred during competition when the speed wasmaximum orclose to maximum.
Besides running,kicking is another activity in which hamstring muscle strain injury frequently occurs.Gabbe etal.5reported that 19%of the confirmed hamstring muscle strain injuries in community level Australian football occurred during kicking while over80%in running orsprinting.Brooks etal.6reported thatabout10%of the hamstring muscle strain injuriesin English rugby occurred during kicking.Brooksetal.6also found that the hamstring muscle strain injuries occurred in kicking were more severe than those occurred in other activities in terms of lost play time.
Several studies have been conducted on the biomechanics of running to better understand the mechanism of hamstring muscle strain injury.Mann and Sprague43,44comprehensively described sagittal plane joint resultant moments in sprinting. The results of their studies demonstrated a peak knee flexion moment and a peak hip extension moment immediately after foot strike,which was suggested as a factor related to the incident of hamstring muscle strain injury.However,previous studies on the general mechanism of muscle strain injury demonstrated that great muscle force was not a necessary condition for a strain injury.
Wood45presented joint resultant moments and power, electromyography(EMG),and hamstring muscle lengths in sprinting.These data confirmed the finding of a peak knee flexion moment and a peak of hip extension moment immediately after the foot strike by Mann and Sprague.43,44These data,however,also demonstrated that knee and hip joint resultant powers were all positive when the peak knee flexion moment and peak hip extension moment occurred immediately after the foot strike.This suggests that the hamstring muscle group is in a concentric contraction after the foot strike,in which a hamstring muscle strain injury is not likely to occur.45The hamstring muscle length and EMG data demonstrated that hamstring muscles were in eccentric contractions during the late swing phase before footstrike and late stance phase before takeoff.45These data suggest that hamstring muscle strain injury may occur before foot strike and before takeoff.
Two recent studies confi rmed the data in the previous study.45Thelen et al.46also found a hamstring muscle eccentric contraction during the late swing phase oftreadmill sprinting,and suggested that the potential for hamstring muscle strain injury existed during the late swing phase.Their results,however,did not show a hamstring muscle eccentric contraction during the stance phase as Wood45did.Yu etal.47analyzed the biomechanics of ground sprinting,and also found that the hamstring was in eccentric contraction during the late swing phase as wellas during the late stance phase as reported by Wood.Yu et al.47suggested that hamstring muscles were atthe risk forstrain injury during the late stance phase as well as during the late swing phase.However, hamstrings may have higher risk for strain injury during the late swing phase than during the late stance phase because the lengths of the hamstring muscles were signifi cantly longer during the late swing phase than during the late stance phase.47
7.Risk factors
Understanding risk factors for hamstring strain injury is criticalfor developing prevention and rehabilitation strategies. Many risk factors forhamstring muscle strain injury have been identified in the literature,however,only a few of these are evidence-based while the majority are theory-based.These risk factors can be categorized as modifiable factors and nonmodifiable factors.48Modifiable risk factors include shortened optimum muscle length,lack of muscle flexibility,strength imbalance,insufficientwarm-up,fatigue,low back injury,and increased muscle neuraltension(Table 1).Non-modifiable risk factors include muscle compositions,age,race,and previous injuries(Table 1).
7.1.Shortened optimum muscle length
Optimum muscle length is defined as the muscle length at which the muscle contractile elementgenerates maximum force, which is similarto the muscle resting length.49,50Brocketetal.51demonstrated that legs with hamstring muscle strain injury histories have a significantly greater knee flexion angle for the maximum knee flexion torque in comparison to legs without hamstring muscle strain injury histories.This means that legs with hamstring muscle strain injury histories may have shorter optimum hamstring muscle lengths and thus higher muscle strains in comparison to legswithoutinjury histories for the same range of motion.This suggests that shortened optimum hamstring muscle length is a risk factor for hamstring strain injury.However,a recent prospective study on risk factors of hamstring injuries in sprinters did not show a significant difference in the knee flexion angle forthe peak knee flexion torque in preseason test between injured and uninjured athletes.52
7.2.Lack of muscle flexibility
Poor muscle flexibility has been repeatedly suggested as a modifiable risk factorformuscle strain injury.A recentstudy provided theoreticalsupportforthis suggestion from a pointof view of the effect of hamstring flexibility on isometric knee flexion angle—torque relationship.53This study demonstrated thatsubjects with poorhamstring flexibility had a greaterknee flexion angle for the maximum knee flexion torque in an isometric contraction test in comparison to subjects with normal hamstring flexibility.This result indicates that an athlete with poor hamstring flexibility may have shorter optimum hamstring muscle lengths in comparison to athletes with normal hamstring flexibility.As previously discussed, shorter optimum muscle length may result in higher muscle strain for the same range of motion,and thus increase the risk for hamstring strain injury.However,the results of clinical studies on the effect of hamstring flexibility on the risk forhamstring muscle strain injury are inconsistent.Worrelletal.54conducted a case-control study in which 16 athletes who had hamstring strain injuries within the past 18 months and 16 sports and dominant leg matched controls without injury were tested for their hamstring flexibility and concentric and eccentric strength at 60°/s and 180°/s.The results showed a significant difference in hamstring flexibility between injured and matched control groups.Two prospective studies indicated that English soccer players who sustained a hamstring muscle injury had significantly less hamstring muscle flexibility measured before their injuries compared to their uninjured counterpart.55,56These studies support poor hamstring flexibility as a risk factor for hamstring muscle strain injury.However,several other studies showed no significant difference in hamstring flexibility prior to hamstring muscle strain injuries between injured and uninjured athletes.52,57—59A study by Gabbe et al.60showed that elite Australian football players who had recurrences of hamstring muscle strain injury appeared to have better hamstring flexibility in comparison to their counterpart without recurrence of the injury.The inconsistency among these studies may be due to differences in control group, controlof other risk factors,and injury risk measures in study designs.Further studies with improved research designs are needed to determine the effects of flexibility on the risk of hamstring muscle strain injury.
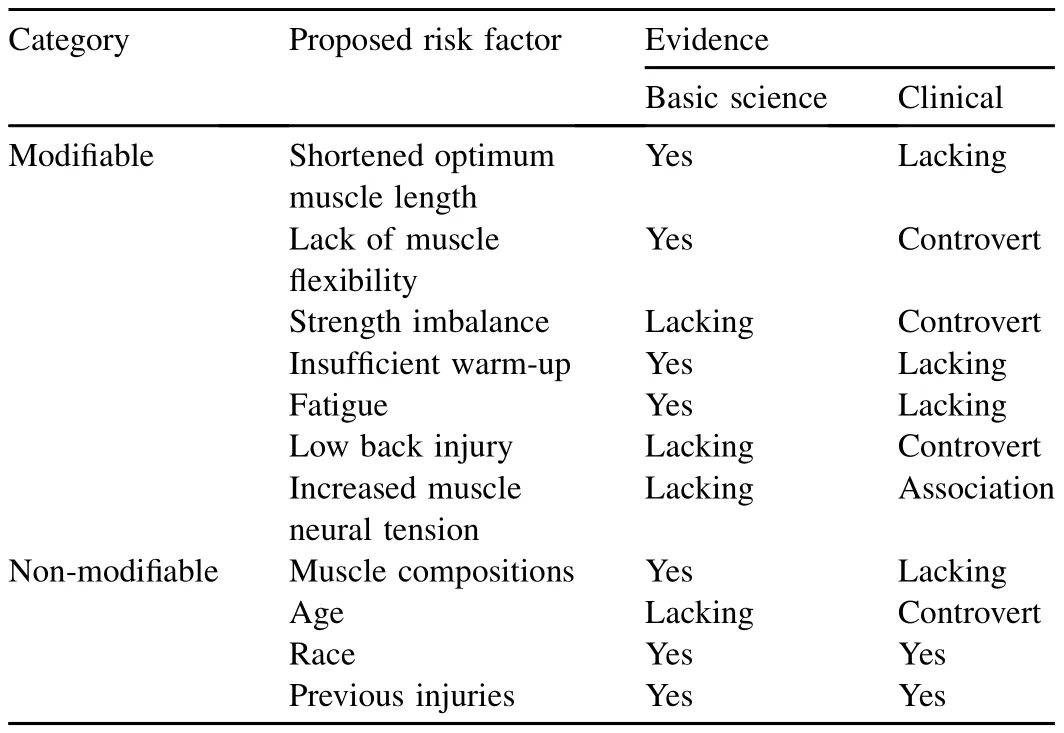
Table 1Proposed risk factors for hamstring muscle strain injury in the literature.
7.3.Hamstring strength imbalance
Hamstring strength imbalance is a commonly proposed modifiable risk factor.Two hamstring strength measures have been used to quantify hamstring strength imbalance:bilateral hamstring strength asymmetry and hamstring to quadriceps strength ratio.Hamstring strength imbalance quantified by either of these two measures is considered a risk factorfor hamstring muscle strain injury.Many prevention programs have been designed in attempt to prevent hamstring muscle strain injury through strength training.This review,however,found that the research results on the role of hamstring strength imbalance played in the risk ofhamstring strain injury are inconsistent.
Orchard et al.59predicted hamstring muscle strain injuries for 62 legs of Australian football players using hamstring strength measures as independent variables.The results showed thatthe injured legs had significantly lower concentric isokinetic hamstring strength and hamstring to quadriceps strength ratio tested ata speed of 60°/s compared to uninjured legs.In addition,injured athletes had significantly lower injured to uninjured concentric isokinetic hamstring strength tested at 60°/s compared to uninjured athletes.However,the sensitivity and specificity of the prediction ofhamstring strain injury from hamstring strength were 28%and 98%,respectively,which means that the hamstring strength had a better prediction of no injury than injury.Croisier et al.61reported a significant difference in the ratio of hamstring eccentric strength tested at30°/s to quadriceps concentric strength tested at 240°/s between a hamstring strain injury recurrence group and a non-recurrence group of soccer,track and field,and martialarts athletes.Croisier etal.62found thatsoccer players with uncorrected preseason hamstring strength imbalance had a significantly higher rate of hamstring strain injury in comparison to those without preseason hamstring strength imbalance,and to those with confirmed correction of preseason hamstring strength imbalance.Sugiura et al.63reported similarresultsforsprintersasthose by Orchard etal.59for Australian football players.Yeung et al.52reported that the hamstring-to-quadriceps concentric strength ratio tested at 180°/s was the best predictor of hamstring strain injury. Fousekis et al.64reported that bilateral hamstring eccentric strength asymmetry was the best predictor of hamstring strain injury for soccer players.Askling et al.65and Petersen et al.66reported that hamstring specific eccentric strength training significantly reduced hamstring injury in Sweden soccer players.
While these studiessupporthamstring strength imbalance as being a risk factor for hamstring strain injury,several other studies showed otherwise.A retrospective case-control study showed no significant difference in hamstring and quadriceps concentric and eccentric strengths,bilateral strength asymmetries,and hamstring to quadriceps strength ratios at 60°/s and 180°/s.54Similarresults were reported in anotherretrospective study.51Although the effectsofrehabilitation on the strength of those injured athletes were unknown in these two studies,the results were consistent with a prospective study.67Two randomized controlled trial studies reported that a hamstring strengthening intervention did notsignificantly reduce the risk for hamstring strain injury.30,60Although investigators of both studies blamed low compliance as the reason for negative results,neither of the studies reported on any other outcome measures of their intervention programs.It is unclear if the negative resultsin injury rates were due to lack of effect of their intervention program on injury rate oron strength.
Future studies are needed to better understand the effects of strength imbalance and strength training on risk of hamstring strain injury.Basic science studies on the general mechanism of muscle strain injuries demonstrate that muscle strain is the primary cause of muscle strain injury,and have established theoretical connections between muscle strain and flexibility and between flexibility and muscle strain injury.However,the theoretical connection between muscle strength and muscle strain injury stillneeds to be established.Future studies should consider multiple factors instead of hamstring strength alone, and emphasize the cause-and-effect relationship between strength and injury.Comparisons of hamstring strength between injured and uninjured groups provide little information on this relationship.The time when hamstring strength is tested may need to be carefully arranged in future studies.Schache etal.68found thatthe bilateralhamstring strength asymmetry significantly increased 5 days priorthe hamstring strain injuries.
7.4.Insufficient warm-up
Insufficient warm-up has also been suggested as a modifiable risk factorforhamstring muscle strain injury due to early observations that many hamstring muscle strain injuries occurred during the early portions of practices or competitions.11This is supported by a study by Safran et al.69that demonstrated thatincreasing muscle temperature increases the muscle length and force atfailure of rabbithind limb muscles. However,a study by Gillette et al.70demonstrated that a 20-min warm-up increased body core temperature but did not increase hamstring flexibility.This review failed to find any clinical studies,which showed that an insufficient warm-up results in an increased hamstring muscle strain injury rate.
7.5.Fatigue
The suggestion that fatigue is a modifiable risk factor for hamstring muscle strain injury was also based on the clinical observation that many hamstring muscle strain injuries occurred during the late portions of practices and competitions.6,8,11This suggestion was supported by a study by Mair etal.71in which the investigators found thatalthough fatigued and non-fatigued muscles failed at the same length,the nonfatigued muscles absorbed significantly less energy before failure.These results indicate thata fatigued athlete may have to increase the elongation to absorb a given amount of energy and thus increased muscle strains in the movementand the risk for muscle strain injury.The study by Small et al.72also provides supportfor fatigue as being a risk factor.They found that fatigue significantly increased the knee flexion angle at which peak knee eccentric flexion torque occurred.This result combined with the results of those studies on the general mechanism of muscle strain injury and optimum hamstring muscle length indicate that hamstring muscle strain may be increased in a given movement when fatigued.To a certain degree,this result also supports increasing hamstring flexibility as a prevention strategy for hamstring strain injury.
7.6.Lumbar disorders
Hamstring strain injury may be associated with low back pain in the zygapophyseal origin area.73Mooney and Robertson74found increased electrical activities and decreased flexibility of hamstring muscles for patients with low back pain.These results indicate that low back pain may provoke hamstring responses such as increased tension and result in muscle damage.73In a retrospective study,Hennessey and Watson75found a significant increase of lumbar lordosis among hamstring injured athletes in comparison to their uninjured counterparts,which indicates a possible association between hamstring strain injury and lumbar posture.However, a study by Verrall et al.2found that a past history of back injury did correlate with an increased risk of posterior thigh pain,which did notnecessarily mean a hamstring strain injury.
7.7.Neuraltension
Abnormal neural tension was another proposed modifiable risk factor for the recurrence of hamstring strain injuries.76Abnormal neural tension is defined as abnormal physiological and mechanical responses in the neuromuscular system when the normalrange ofmovementand stretch capabilities is exceeded.77,78Neural tension can be evaluated using the Slump test.77,78Branches of the sciatic nerve can be tethered to the scar after a hamstring injury,and create increased neural tension with or without local irritation,which may result in local damage to the hamstring muscle.73Turl and George76reported that more than 50%of athletes had abnormalneural tension after non-repetitive grade I hamstring strain injuries. However,as previous studies on the mechanism of muscle strain injury demonstrated,muscle strain injuries are caused by strain,notby force.35,36As the relationship between muscle strain injury and abnormalneuraltension is stillspeculative in nature,the relevance of incorporating special mobility techniques including“neural tension positions”in rehabilitation programs has not yet been scientifically established.29
7.8.Muscle fiber composition
Several basic science studies have demonstrated that Type II(fast)muscle fibers were more prone to strain injury than Type I(slow)muscle fibers.Garrett et al.79noticed that muscles prone to strain injury have more Type II fibers than muscles notprone to strain injury,and thathamstring muscles have a relatively high percentage of Type Ifibers compared to other lower extremity muscles.They hypothesized that muscles comprised of a high percentage of fast fibers were prone to strain injury.This hypothesis has been supported by basic science studies.Friden and Lieber80demonstrated that eccentric contraction-induced strain injuries predominantly occurred in fast fibers with low oxidative capacity.They hypothesized that oxidative capacity was an important factor that affects the eccentric contraction induced muscle injury. Macpherson et al.81demonstrated that fast fibers had more severe strain injury with less strain in comparison to slow fibers.These results combined together indicate that athletes with a higher percentage of type I fibers may be prone to hamstring strain injury as well as other muscle strain injuries.No clinical studies have been found to support this hypothesis.
7.9.Age
Many retrospective and prospective studies have identified age as a risk factor of hamstring strain injury.Orchard et al.82found that Australian footballplayers older than 23 years had a significantly higher risk for hamstring strain injuries than playersyoungerthan 23 years.Woodsetal.8and Ekstrand etal.24reported similar results for English and European soccer players.Gabbe et al.5,60reported that Australian football players older than 25 years sustained more hamstring strain injuries than did their younger counterparts.Verrall et al.2estimated that an increase of 1 year in age increased hamstring strain injury rate by 1.3 times for Australian football players,while Henderson et al.83estimated that the odds for sustaining hamstring injury increased 1.78 times for each 1 year increase in age for English soccer players.The studies on the hamstring strain injury in rugby and Australian footballdid notshow significantly effectof age on hamstring strain injury rate.6,84
Orchard etal.82attributed the association between age and the risk for hamstring strain injury to the decrease in hamstring strength induced by hamstring muscle fiber denervation due to L5 and S1 never impingement caused by age-related low lumbardegeneration.He argued thatthe decrease in hamstring strength as quadricep strength remained unchanged would result in a hamstring strength imbalance relative to the quadricep strength,and thus increased the risk for hamstring strain injury.82Orchard et al.’s explanation of the mechanism of the age effecton the risk of hamstring strain injury was based on the theory thatmuscle strength is a risk factorformuscle strain injury,which has not been validated by basic science and clinical studies.In addition,Orchard et al.’s study82did not demonstrate any difference in hamstring strength between their old and young subjects.Gabbe etal.60found age related differences in body weight,hip flexor flexibility,and ankle plantarflexor flexibility,butcould notexplain the connections between these age-related differences and age-related differences in hamstring strain injury rate.
7.10.Race
Differenthamstring injury rates in athletes ofdifferentraces have been repeatedly reported in the literature.Verrall et al.2found that Australian football players who were of aboriginal descent had a significantly higher risk of hamstring injuries in comparison to players ofotherraces.Woodsetal.8reported that English professional soccer players of African descent have a significantly higher risk of hamstring strain injury in comparison to players of other races.Brooks et al.6noticed that, although notstatistically significant,the incidence of hamstring strain injury among African and Caribbean descents was almost four times that of Caucasian players.These results suggestthat individuals of difference races may have differentmuscle fiber compositions.Ama et al.85demonstrated that individuals of African descent have more fast fibers than Caucasians.As previously mentioned,athleteswho have more fastfibersmay be prone to muscle strain injury.Woods etal.8also argued thatthe increased pelvis anterior tilt of African descents might be anotherexplanation oftheirelevated hamstring strain injury risk. However,a study by Mosneretal.86found no difference in actual pelvis anterior tiltbetween African and Caucasian individuals.
7.11.Previous hamstring injury
Many studies have demonstrated thata history of hamstring strain injury is a significantrisk factor for the recurrence of the injury.2,4,6,60,67,87—89Engebretsen et al.58suggested that previous injury was the only significant risk factor for new hamstring strain injury for a group of Norwegian soccer players.Based on an animal experiment,Nikolaou et al.37suggested that scarring and fibrosis seen in the muscle 7 days after initial strain injury may explain the elevated risk of the injury.As previously mentioned,Brockett et al.51demonstrated that the legs with hamstring muscle strain injury histories had a significantly greater knee flexion angle forthe maximum knee flexion torque in comparison to the legs without hamstring muscle strain injury histories.This indicates a possibility that previous strain injury resulted in shortened optimum lengths of hamstring muscles and thus increased the risk for injury.However,a recent prospective study by Fousekis et al.64reported that previous hamstring injury significantly decreased the odds of injury.A possible explanation for this resultis thatrehabilitation programs might have eliminated some risk factors or reduced the effects of risk factors for the subjects involved.
Besides the above mentioned risk factors,a study by Sherry and Best90showed that poor agility and trunk stabilization may be risk factors for hamstring muscle strain injury while a study by Cibulka et al.91showed that sacroiliac joint dysfunction may also be a risk factor.However,similar to many previously discussed risk factors,the scientific basis of these proposed risk factors is not clear.
8.Summary
Hamstring strain injury is one of the most common sports injuries that have significant effects on patients’quality of life and sports career.The high recurrence rate and serious consequences of this injury have not been fully recognized.
Basic science studies have demonstrated that the excessive strain during an eccentric contraction is the general mechanism of muscle strain injury,and that the severity of the injury is affected by the eccentric contraction speed when the muscle strain is large and by the duration of activation before the eccentric contraction.In vivo studies demonstrated that hamstring injury is likely to occur during the late swing phase of sprinting when the knee is extending and the hip is flexed and during the late stance phase before takeoff when knee is extending and the trunk is leaning forward.
Many risk factors including poor flexibility,strength imbalance,insufficient warm-up,and fatigue have been proposed as risk factors for hamstring strain injury.Basic science studies have established the connections between muscle strain and strain injury,muscle optimum length and muscle strain,and flexibility and muscle optimum length, which supportpoor flexibility and insufficient warm-up as risk factors for hamstring strain injury.However,the theoretical basis of hamstring strength imbalance and other proposed risk factors for hamstring strain injury is lacking.
Many clinical studies have been conducted in attempts to provide clinicalevidence to supportthe proposed risk factors. However,the results of those clinical studies are descriptive and controversial.Clinicalevidence for currentprevention and rehabilitation programs for hamstring injury is lacking.
Future studies are needed to improve the prevention and rehabilitation ofhamstring strain injury,particularly randomized controlled trials,in order to establish the cause-and-effectrelationships between those proposed risk factors and hamstring strain injury.Future clinicalresearch should consider the interaction effects of multiple risk factors on the risk of hamstring strain injury.Clinicalstudies on risk factors and prevention and rehabilitation programs should be based on the injury mechanisms established in basic science studies.Evidence-based prevention and rehabilitation programs for hamstring strain injuries can be developed only after risk factors of the injury have been scientifically identified,confirmed,and understood through well-designed basic science and clinicalstudies.
1.Verrall GM,Slavotinek JP,Barnes PG.The effect of sports specific training on reducing the incidence of hamstring injuries in professional Australian rules football players.Br J Sports Med 2005;39:363—8.
2.VerrallGM,Slavotinek JP,Barnes PG,Fon GT,Spriggins AJ.Clinicalrisk factors for hamstring muscle strain injury:a prospective study with correlation of injury by magnetic resonance imaging.Br J Sports Med 2001;35:435—9.discussion 440.
3.Orchard J,Seward H.Epidemiology of injuries in the Australian football league,seasons 1997—2000.Br J Sports Med 2002;36:39—44.
4.Hoskins WT,Pollard H.Injuries in Australian rules football.A review of the literature.Australas Chiropr Osteopat 2003;11:49—56.
5.Gabbe BJ,Finch CF,Bennell KL,Wajswelner H.Risk factors for hamstring injuries in community level Australian football.Br J Sports Med 2005;39:106—10.
6.Brooks JH,Fuller CW,Kemp SP,Reddin DB.Incidence,risk,and prevention ofhamstring muscle injuries in professionalrugby union.Am J Sports Med 2006;34:1297—306.
7.Woods C,Hawkins RD,Hulse M,Hodson A.The football association medicalresearch programme:an audit of injuries in professionalfootball—analysis of preseason injuries.Br J Sports Med 2002;36:436—41.
8.Woods C,Hawkins RD,Maltby S,Hulse M,Thomas A,Hodson A.The football association medical research programme:an audit of injuries in professional football—analysis of hamstring injuries.Br J Sports Med 2004;38:36—41.
9.Arnason A,Andersen TE,Holme I,Engebretsen L,Bahr R.Prevention of hamstring strains in elite soccer:an intervention study.Scand J Med Sci Sports 2008;18:40—8.
10.Dadebo B,White J,George KP.A survey of flexibility training protocols and hamstring strains in professional football clubs in England.Br J Sports Med 2004;38:388—94.
11.Ekstrand J,Gillquist J.The frequency of muscle tightness and injuries in soccer players.Am J Sports Med 1982;10:75—8.
12.Brophy RH,Chehab EL,Barnes PG,Lyman S,Rodeo SA,Warren RF. Predictive value of orthopedic evaluation and injury history at the NFL combine.Med Sci Sports Exerc 2008;40:1368—72.
13.Feeley BT,Kennelly S,Barnes RP,Muller MS,Kelly BT,Rodeo SA,etal. Epidemiology of national football league training camp injuries from 1998 to 2007.Am J Sports Med 2008;36:1597—603.
14.Elliott MC,Zarins B,Powell JW,Kenyon CD.Hamstring muscle strains in professional football players:a 10-year review.Am J Sports Med 2011;39:843—50.
15.Chakravarthy J,Ramisetty N,Pimpalnerkar A,MohtadiN.Surgicalrepair of complete proximal hamstring tendon ruptures in water skiers and bull riders:a reportof four cases and review of the literature.Br J Sports Med 2005;39:569—72.
16.Connell DA,Schneider-Kolsky ME,Hoving JL,Malara F,Buchbinder R, Koulouris G,et al.Longitudinal study comparing sonographic and MRI assessments of acute and healing hamstring injuries.AJR Am J Roentgenol2004;183:975—84.
17.De Smet AA,Best TM.MR imaging of the distribution and location of acute hamstring injuries in athletes.AJR Am J Roentgenol 2000;174:393—9.
18.Koulouris G,Connell D.Evaluation of the hamstring muscle complex following acute injury.Skeletal Radiol 2003;32:582—9.
19.Kurosawa H,Nakasita K,Nakasita H,Sasaki S,Takeda S.Complete avulsion of the hamstring tendons from the ischialtuberosity.A reportof two cases sustained in judo.Br J Sports Med 1996;30:72—4.
20.Sallay PI,Friedman RL,Coogan PG,Garrett WE.Hamstring muscle injuries among water skiers.Functional outcome and prevention.Am J Sports Med 1996;24:130—6.
21.Sarimo J,Lempainen L,Mattila K,Orava S.Complete proximal hamstring avulsions:a series of41 patients with operative treatment.Am J Sports Med 2008;36:1110—5.
22.Askling C,Lund H,Saartok T,Thorstensson A.Self-reported hamstring injuries in student-dancers.Scand J Med Sci Sports 2002;12:230—5.
23.Hawkins RD,Hulse MA,Wilkinson C,Hodson A,Gibson M.The association football medical research programme:an audit of injuries in professional football.Br J Sports Med 2001;35:43—7.
24.Ekstrand J,Hagglund M,Walden M.Epidemiology of muscle injuries in professional football(soccer).Am J Sports Med 2011;39:1226—31.
25.Orchard J,Best TM.The management of muscle strain injuries:an early return versus the risk of recurrence.Clin J Sport Med 2002;12:3—5.
26.Clanton TO,Coupe KJ.Hamstring strains in athletes:diagnosis and treatment.J Am Acad Orthop Surg 1998;6:237—48.
27.Petersen J,Holmich P.Evidence based prevention of hamstring injuries in sport.Br J Sports Med 2005;39:319—23.
28.Ekstrand J,Healy JC,Walden M,Lee JC,English B,Hagglund M. Hamstring muscle injuries in professionalfootball:the correlation of MRI findings with return to play.Br J Sports Med 2012;46:112—7.
29.Croisier JL.Factors associated with recurrent hamstring injuries.Sports Med 2004;34:681—95.
30.Gidwani S,Bircher MD.Avulsion injuries of the hamstring origin—a series of 12 patients and management algorithm.Ann R Coll Surg Engl 2007;89:394—9.
31.Askling CM,Tengvar M,Saartok T,Thorstensson A.Acute first-time hamstring strains during high-speed running:a longitudinal study including clinical and magnetic resonance imaging findings.Am J Sports Med 2007;35:197—206.
32.Muckle DS.Associated factors in recurrent groin and hamstring injuries. Br J Sports Med 1982;16:37—9.
33.Hernesman SC,Hoch AZ,Vetter CS,Young CC.Footdrop in a marathon runner from chronic complete hamstring tear.Clin J Sport Med 2003;13:365—8.
34.Petersen J,Thorborg K,Nielsen MB,Holmich P.Acute hamstring injuries in Danish elite football:a 12-month prospective registration study among 374 players.Scand J Med Sci Sports 2010;20:588—92.
35.Garrett WE,Safran MR,Seaber AV,Glisson RR,Ribbeck BM.Biomechanical comparison of stimulated and nonstimulated skeletal muscle pulled to failure.Am J Sports Med 1987;15:448—54.
36.Lieber RL,Friden J.Muscle damage is nota function ofmuscle force but active muscle strain.J Appl Physiol 1993;74:520—6.
37.Nikolaou PK,Macdonald BL,Glisson RR,Seaber AV,Garrett WE. Biomechanical and histological evaluation of muscle after controlled strain injury.Am J Sports Med 1987;15:9—14.
38.Best TM,McElhaney JH,Garrett Jr WE,Myers BS.Axial strain measurements in skeletal muscle at various strain rates.J Biomech Eng 1995;117:262—5.
39.Brooks SV,Faulkner JA.Severity ofcontraction-induced injury is affected by velocity only during stretches of large strain.J Appl Physiol 2001;91:661—6.
40.Lovering RM,Hakin M,Moorman CT,De Deyne PG.The contribution of contractile pre-activation to loss of function after a single lengthening contraction.J Biomech 2005;38:1501—7.
41.Garrett Jr WE.Muscle strain injuries.Am J Sports Med 1996;24:S2—8.
42.VerrallGM,Slavotinek JP,Barnes PG,Fon GT.Diagnostic and prognosticvalue of clinical findings in 83 athletes with posterior thigh injury:comparison of clinicalfindingswith magnetic resonance imaging documentation ofhamstring muscle strain.Am J Sports Med 2003;31:969—73.
43.Mann R,Sprague P.A kinetic analysis of the ground leg during sprint running.Res Q Exerc Sport 1980;51:334—48.
44.Mann RV.A kinetic analysis of sprinting.Med Sci Sports Exerc 1981;13:325—8.
45.Wood GA.Biomechanical limitations to sprint running.Med Sport Sci 1987;25:58—71.
46.Thelen DG,Chumanov ES,Best TM,Swanson SC,Heiderscheit BC. Simulation of biceps femoris musculotendon mechanics during the swing phase of sprinting.Med Sci Sports Exerc 2005;37:1931—8.
47.Yu B,Queen RM,Abbey AN,Liu Y,Moorman CT,Garrett WE. Hamstring muscle kinematics and activation during overground sprinting. J Biomech 2008;41:3121—6.
48.Clark RA.Hamstring injuries:risk assessmentand injury prevention.Ann Acad Med Singap 2008;37:341—6.
49.Hatze H.Myocybernetic control models of skeletal muscle.Pretoria: University of South Africa;1981.
50.Kaufman FR,An KN,Chao EY.Incorporation ofmuscle architecture into muscle length—tension relationship.J Biomech 1989;22:943—8.
51.Brocket CL,Morgan DL,Proske U.Predicting hamstring strain injury in elite athletes.Med Sci Sports Exerc 2004;36:379—87.
52.Yeung SS,Suen AM,Yeung EW.A prospective cohortstudy of hamstring injuries in competitive sprinters:preseason muscle imbalance as a possible risk factor.Br J Sports Med 2009;43:589—94.
53.Alonso J,McHugh MP,Mullaney MJ,Tyler TF.Effect of hamstring flexibility on isometric knee flexion angle-torque relationship.Scand J Med Sci Sports 2009;19:252—6.
54.Worrell TW,Perrin DH,Gansneder BM,Gieck JH.Comparison of isokinetic strength and flexibility measures between hamstring injured and noninjured athletes.J Orthop Sports Phys Ther 1991;13:118—25.
55.Bradley PS,Olsen PD,Portas MD.The effect of static,ballistic,and proprioceptive neuromuscular facilitation stretching on vertical jump performance.J Strength Cond Res 2007;21:223—6.
56.Witvrouw E,DanneelsL,Asselman P,D’Have T,CambierD.Muscleflexibility as a risk factor for developing muscle injuries in male professional soccer players.A prospective study.Am J Sports Med 2003;31:41—6.
57.Burkett LN.Causative factors in hamstring strains.Med Sci Sports 1970;2:39—42.
58.Engebretsen AH,Myklebust G,Holme I,Engebretsen L,Bahr R.Intrinsic risk factors for hamstring injuries among male soccer players:a prospective cohort study.Am J Sports Med 2010;38:1147—53.
59.Orchard J,Marsden J,Lord S,Garlick D.Preseason hamstring muscle weakness associated with hamstring muscle injury in Australian footballers.Am J Sports Med 1997;25:81—5.
60.Gabbe BJ,Bennell KL,Finch CF,Wajswelner H,Orchard JW.Predictors of hamstring injury at the elite levelof Australian football.Scand J Med Sci Sports 2006;16:7—13.
61.Croisier JL,Forthomme B,Namurois MH,Vanderthommen M, Crielaard JM.Hamstring muscle strain recurrence and strength performance disorders.Am J Sports Med 2002;30:199—203.
62.Croisier JL,Ganteaume S,Binet J,Genty M,Ferret JM.Strength imbalances and prevention of hamstring injury in professional soccer players:a prospective study.Am J Sports Med 2008;36:1469—75.
63.Sugiura Y,Saito T,Sakuraba K,Sakuma K,Suzuki E.Strength deficits identified with concentric action of the hip extensors and eccentric action of the hamstrings predispose to hamstring injury in elite sprinters. J Orthop Sports Phys Ther 2008;38:457—64.
64.Fousekis K,Tsepis E,Poulmedis P,Athanasopoulos S,Vagenas G. Intrinsic risk factors of non-contact quadriceps and hamstring strains in soccer:a prospective study of 100 professional players.Br J Sports Med 2011;45:709—14.
65.Askling C,Karlsson J,Thorstensson A.Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload.Scand J Med Sci Sports 2003;13:244—50.
66.Petersen J,Thorborg K,Nielsen MB,Budtz-Jørgensen E,Hölmich P. Preventive effectofeccentric training on acute hamstring injuries in men’s soccer:a cluster-randomized controlled trial.Am J Sports Med 2011;39:2296—303.
67.Bennell K,Wajswelner H,Lew P,Schall-Riaucour A,Leslie S,Plant D, et al.Isokinetic strength testing does not predict hamstring injury in Australian rules footballers.Br J Sports Med 1998;32:309—14.
68.Schache AG,Crossley KM,Macindoe IG,Fahrner BB,Pandy MG.Can a clinical test of hamstring strength identify football players at risk of hamstring strain?Knee Surg Sports Traumatol Arthrosc 2011;19:38—41.
69.Safran MR,GarrettWEJ,SeaberAV,Glisson RR,Ribbeck BM.The role of warmup in muscular injury prevention.Am J Sports Med 1988;16:123—9.
70.Gillette TM,Holland GJ,Vincent WJ,Loy SF.Relationship of body core temperature and warm-up to knee range of motion.J Orthop Sports Phys Ther 1991;13:126—31.
71.Mair SD,Seaber AV,Glisson RR,Garrett WE.The role offatigue in susceptibility to acute muscle strain injury.Am J Sports Med 1996;24:137—43.
72.Small K,McNaughton L,Greig M,Lovell R.The effects of multidirectional soccer-specific fatigue on markers of hamstring injury risk.J Sci Med Sport 2010;13:120—5.
73.Devlin L.Recurrentposteriorthigh symptoms detrimentalto performance in rugby union:predisposing factors.Sports Med 2000;29:273—87.
74.Mooney V,Robertson J.The facet syndrome.Clin Orthop Relat Res 1976;115:149—56.
75.Hennessey L,Watson AW.Flexibility and posture assessment in relation to hamstring injury.Br J Sports Med 1993;27:243—6.
76.Turl SE,George KP.Adverse neural tension:a factor in repetitive hamstring strain?J Orthop Sports Phys Ther 1998;27:16—21.
77.Newsham K.The role of neuraltension in minor and recurrenthamstring injury,part 1:evaluation.Athl Ther Today 2006;11(4):54—6.
78.Newsham K.The role of neural tension in hamstring injury,part 2: treatmentand rehabilitation.Athl Ther Today 2006;11(9):66—9.
79.Garrett Jr WE,Califf JC,Bassett 3rd FH.Histochemical correlates of hamstring injuries.Am J Sports Med 1984;12:98—103.
80.Friden J,Lieber RL.Structural and mechanical basis of exercise-induced muscle injury.Med Sci Sports Exerc 1992;24:521—30.
81.Macpherson PC,Schork MA,Faulkner JA.Contraction-induced injury to single fiber segments from fast and slow muscles of rates by single stretches.Am J Physiol1996;271:C1438—46.
82.Orchard J,SteetE,Walker C,Ibrahim A,Rigney L,Houang M.Hamstring muscle strain injury caused by isokinetic testing.Clin J Sport Med 2001;11:274—6.
83.Henderson G,Barnes CA,Portas MD.Factors associated with increased propensity for hamstring injury in English premier league soccer players. J Sci Med Sport 2010;13:397—402.
84.Koulouris G,Connell DA,Brukner P,Schneider-Kolsky M.Magnetic resonance imaging parameters for assessing risk of recurrent hamstring injuries in elite athletes.Am J Sports Med 2007;35:1500—6.
85.Ama PF,Simoneau JA,Boulay MR,Serresse O,Theriault G,Bouchard C. Skeletal muscle characteristics in sedentary black and Caucasian males. J Appl Physiol 1986;61:1758—61.
86.Mosner EA,Bryan JM,Stull MA,Shippee R.A comparison of actualand apparent lumbar lordosis in black and white adult females.Spine(Phila Pa 1976)1989;14:310—4.
87.Orchard JW.Intrinsic and extrinsic risk factors for muscle strains in Australian football.Am J Sports Med 2001;29:300—3.
88.Upton PA,Noakes TD,Juritz JM.Thermal pants may reduce the risk of recurrenthamstring injuries in rugby players.Br J Sports 1996;30:57—60.
89.Warren P,Gabbe BJ,Schneider-Kolsky M,Bennell KL.Clinical predictors of time to return to competition and of recurrence following hamstring strain in elite Australian footballers.Br J Sports Med 2010;44:415—9.
90.Sherry MA,Best TM.A comparison of 2 rehabilitation programs in the treatment of acute hamstring strains.J Orthop Sports Phys Ther 2004;34:116—25.
91.Cibulka MT,Rose SJ,Delitto A,Sinacore DR.Hamstring muscle strain treated by mobilizing the sacroiliac joint.Phys Ther 1986;66:1220—3.
Received 6 April 2012;revised 25 May 2012;accepted 14 June 2012
*Corresponding author.
E-mailaddress:uncbyu@gmail.com(B.Yu)
Peer review under responsibility of Shanghai University of Sport
Production and hosting by Elsevier
2095-2546/$-see front matter Copyright©2012,Shanghai University of Sport.Production and hosting by Elsevier B.V.All rights reserved. http://dx.doi.org/10.1016/j.jshs.2012.07.003
杂志排行

Journal of Sport and Health Science的其它文章
- Noise-enhanced dynamic single leg balance in subjects with functional ankle instability
- Prevention and rehabilitation of sports injuries
- Exercise in type 2 diabetes:The mechanisms of resistance and endurance training☆
- Endurance tests are the most reliable core stability related measurements
- Do ankle braces provide similar effects on ankle biomechanical variables in subjects with and without chronic ankle instability during landing?
- Anthropometrics and electromyography as predictors for maximal voluntary isometric arm strength